
AUTISMO TEA PDF

TRASTORNO ESPECTRO AUTISMO y URGENCIAS PDF
We Support The Free Share of the Medical Information

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Niveles de Alerta Antiterrorista en España. Nivel Actual 4 de 5.

Fuente Ministerio de Interior de España
sábado, 20 de abril de 2019

viernes, 19 de abril de 2019
Guia para la atención a las personas con discapacidad intelectual o del desarrollo y alteraciones de la salud mental y/o del comportamiento. pdf Gratis
 |
| Guia para la atención a las personas con discapacidad intelectual o del desarrollo y alteraciones de la salud mental y/o del comportamiento. pdf Gratis |
Enlace para DESCARGAR pdf Gratis
https://www.facebook.com/pg/DrRamonReyesMD/photos/?tab=album&%3Balbum_id=620883388254594
Dr. Ramon Reyes, MD
http://emssolutionsint.blogspot.com.es/2016/12/dr-ramon-reyes-diaz-md-emt-t-dmo.html
Les Esperamos en nuestro Grupo en TELEGRAM Soc. IberoAmericana de Emergencias
https://t.me/joinchat/GRsTvEHYjNLP8yc6gPXQ9Q
jueves, 18 de abril de 2019

miércoles, 17 de abril de 2019
WHO guideline recommendations on digital interventions for health system strengthening free PDF

Publication details
Number of pages: 124
Publication date: 2019
Languages: English
ISBN: 978-92-4-155050-5
Publication date: 2019
Languages: English
ISBN: 978-92-4-155050-5
DOWNLOAD
- WHO Guideline: recommendations on digital interventions for health system strengthening
pdf, 1,3Mb - Executive summary
- Web supplement 1: evidence-to-decision frameworks
- Research considerations
- Evidence and recommendations
The key aim of this guideline is to present recommendations based on a critical evaluation of the evidence on emerging digital health interventions that are contributing to health system improvements, based on an assessment of the benefits, harms, acceptability, feasibility, resource use and equity considerations. For the purposes of this version of the guideline, the recommendations examine the extent to which digital health interventions available via mobile devices are able to address health system challenges at different layers of coverage along the pathway to universal health coverage (UHC). By reviewing the evidence of different digital interventions, as well as assessing the risks against comparative options, this guideline aims to equip health policy-makers and other stakeholders with recommendations and implementation considerations for making informed investments into digital health interventions.
This guideline urges readers to recognize that digital health interventions are not a substitute for functioning health systems, and that there are significant limitations to what digital health is able to address.

lunes, 15 de abril de 2019
Incorporating Active Shooter Incident Planning into Health Care Facility Emergency Operations Plans

DOWNLOAD

Fire/Emergency Medical Services Department Operational Considerations and Guide for Active Shooter and Mass Casualty Incidents FEMA
 |
| Fire/Emergency Medical Services Department Operational Considerations and Guide for Active Shooter and Mass Casualty Incidents FEMA |
First Responder Guide for Improving Survivability in Improvised Explosive Device and/or Active Shooter Incidents / Guía DHS para mejorar la supervivencia de primeros respondientes a un incidente a dispositivo explosivo improvisado y tiroteos activos
 |
| First Responder Guide for Improving Survivability in Improvised Explosive Device and/or Active Shooter Incidents / Guía DHS para mejorar la supervivencia de primeros respondientes a un incidente de dispositivo explosivo improvisado y tiroteos activos |
Link to download PDF for Free
FREE PDF: First Responder Guide for Improving Survivability in Improvised Explosive Device and/or Active Shooter Incidents / Guía DHS para mejorar la supervivencia de primeros respondientes a un incidente a dispositivo explosivo improvisado y tiroteos activos
Bajar en el enlace http://goo.gl/L7J3LR
Cortesía
EMS España / Emergency Medical Services en España
Follow me / INVITA A TUS AMIGOS A SEGUIRNOS
https://www.facebook.com/

UNTIL THE HELP ARRIVE instructor guide Version 2.0 by FEMA Uniformed Services University PPT and PDf

Until Help Arrives
- for the Until Help Arrives course, designed to teach students basic skills to keep people with life-threatening injuries alive until professional help arrives.








Tactical Emergency Medical Support (TEMS) Protocols Prehospital Emergency Care Protocols Homeland Security free Pdf

Link to DOWNLOAD
jueves, 11 de abril de 2019
The LTP (Lateral Trauma Position) Why Should You Put Some Trauma Patients on Their Side?
 |
| The LTP (Lateral Trauma Position) Why Should You Put Some Trauma Patients on Their Side? |
The LTP (Lateral Trauma Position)
2015 New Hampshire EMS Protocol 4.5 – Spinal Trauma says, “Patients with nausea or vomiting may be placed in a lateral recumbent position. Maintain neutral head position with manual stabilization, padding/pillows, and/or patient’s arm.” The protocol cited above gives us the option to put a patient on their side while maintaining neutral head position in a situation involving nausea or vomiting.
2015 New Hampshire EMS Protocol 4.5 – Spinal Trauma says, “Patients with nausea or vomiting may be placed in a lateral recumbent position. Maintain neutral head position with manual stabilization, padding/pillows, and/or patient’s arm.” The protocol cited above gives us the option to put a patient on their side while maintaining neutral head position in a situation involving nausea or vomiting.
One of the technique is the Norwegian Lateral Trauma Position (LTP). The goal is to transport a trauma patient who is at risk for airway compromise on their side while making reasonable attempts to maintain inline stabilization of the spine and minimize movement.
Don’t do things without authorization from protocols, medical direction, administration – and you know, the legal stuff.
Don’t do things without authorization from protocols, medical direction, administration – and you know, the legal stuff.
Why Should You Put Some Trauma Patients on Their Side?
Our practice in EMS for decades has been to strap trauma patients to a rigid longboard in a supine position. This has been thought to protect the spine from further injury. We’ve all gotten pretty good at performing that technique, so we’re comfortable doing it.
Unfortunately that comfort is not shared by the patient. Being secured to a ongboard is not comfortable, it’s painful, and it can cause harm to the patient. Furthermore, there is no evidence that it actually makes a difference in patient outcome. So numerous EMS leaders are creating a sea change in EMS across the USA to stop using rigid longboards in the transport of trauma patients.
In 2014-2015 statewide protocols in several New England states took longboards out of the routine care for patients with potential or actual spine trauma. Anecdotal evidence to this point looks very good. However, did we give up anything useful by stopping the practice of transporting patients strapped to a backboard? Let’s think about airway management for a minute. Picture this, you’re in the back of the ambulance with a patient on a backboard. The patient starts to vomit. A lot. How did you manage that? Your suction device wasn’t going to help in this scenario, so as quickly as you could you undid the straps and rolled the patient and backboard up on its side. Gravity then saved the day.
Same scenario, but now we’re NOT transporting the patient on the backboard. How can you roll this patient up on their side and still maintain alignment of the spine? You probably can’t. However airway and breathing come before disability so you do the best you can.
Our state protocols recognize this potential scenario, and say if you think your patient is at risk for vomiting, you should transport them on their side. The language from the 2015 New Hampshire EMS Protocol 4.5 – Spinal Trauma says, “Patients with nausea or vomiting may be placed in a lateral recumbent position. Maintain neutral head position with manual stabilization, padding/pillows, and/or patient’s arm.”
But, but, but, I can’t do that… a trauma patient HAS to be transported supine. Right?
Dogma is defined by the Merriam-Webster dictionary as “a belief or set of beliefs that is accepted by the members of a group without being questioned or doubted”. Maybe the paradigm of transporting every trauma patient in a supine position is dogma that needs to be reconsidered.
The protocol cited above gives us the option to put a patient on their side while maintaining neutral head position in a situation involving nausea or vomiting. This means proactively doing so before initiating transport. THIS IS A VERY GOOD IDEA. There are clearly patients that you can anticipate that vomiting may be in their near future, and you should proactively take steps to deal with it. If endotracheal intubation with RSI, is in your scope of practice that may be the path you take, but transporting the patient on their side may be just as effective and certainly less invasive.
So again, putting a trauma patient who is at risk for aspiration on their side for transport rather than transporting them supine is a very good idea. However we need to do this in a manner that still maintains an inline stabilization of the spine. How do you do that? Good question.
That’s the challenge this project seeks to address. We would like to have a technique that can accomplish that objective.
The Norwegian Lateral Trauma Position
Fortunately our EMS colleagues in Norway developed and have been utilizing a technique called the Lateral Trauma Position for over a decade, with success. What we seek to do here at the LateralTraumaPosition.org project is to take what the Norwegian EMS system started, and help our EMS colleagues in the USA develop this skill. We hope to provide you with information that can help you form your own clinical opinion and your own clinical practice.
This website includes a video that was produced by EMS providers in Norway illustrating the lateral trauma position (LTP) as they practice it. We’ve also included research studies that attempt to determine the effectiveness and safety of the technique. We believe that our practice in EMS should be based on evidence when possible. The current evidence on the LTP isn’t that strong, no randomized controlled trials. But the evidence is growing. This is thanks to the leadership of Dr. Per Kristian Hyldmo, a flight physician for the helicopter EMS system in Norway. We highly admire his work and hope to follow in his footsteps.
The demonstration videos in this website show the LTP as we have worked out the bugs for us. We wouldn’t presume to say this is the only way to do it. What we do say is that EMS providers need to practice a technique that accomplishes the goal, which is to transport a trauma patient who is at risk for airway compromise on their side while making reasonable attempts to maintain inline stabilization of the spine and minimize movement.
We suggest your team starts with our techniques, modifies the techniques to what works for you, then practice it. A lot.
Listen, for years and years we practiced the PHTLS technique of a standing takedown onto a long backboard, right? Well our evolving practice appears to be doing away with that technique, but we should practice the new LTP technique with the same fervor.
So we ask you to review our “how to” videos, practice them with your crews, modify them to suit your needs and your equipment, and get really good at it. We’d really appreciate your feedback and your modifications of the techniques, including photos and videos.
Finally, understand that we’re not holding ourselves out as experts on the topic of spinal immobilization. We are not researchers. We are simply partners in trying to develop an effective technique in the setting of changing protocols and clinical practices.
Oh, and don’t do things without authorization from protocols, medical direction, administration – you know, the legal stuff.
Be safe,
The LateralTraumaPosition.org Team
- Evidence / Research Protocols
- Protocols – Spinal Motion Restriction Protocol – State of Connecticut EMS
- Protocols – Spinal Motion Restriction Protocol – State of Vermont EMS
- Research – Hyldmo, et. al.; Systematic Review of Airway Compromise and Supine Position
- Research – PCRF Journal Club Review of Article About Loss of Airway Patency in Unconscious Supine Patients
- Research – Hyldmo, et. al. – Safety of the Lateral Trauma Position: A Cadaver Model Study – Acta Anaesthesiologica Scandinavica
- Español Posicion Lateral de Seguridad PLS by Emergentziak Osakidetza
-
SUBITUS International@SUBITUSINT #SUBITUSINT+1 849-849-8576+34 671454059subitusint@gmail.com


Daños de un atropeyo segun la velocidad. Infografia
 |
| Daños de un atropeyo segun la velocidad. Infografia |
Ley No. 63-17, de Movilidad, Transporte Terrestre, Tránsito y Seguridad Vial de la República Dominicana. G. O. No. 10875 del 24 de febrero de 2017.
https://emssolutionsint.blogspot.com/2019/01/ley-no-63-17-de-movilidad-transporte.html

SUBITUS International
@SUBITUSINT #SUBITUSINT
+1 849-849-8576
+34 671454059
sábado, 6 de abril de 2019

Enlace para DESCARGAR

SUBITUS International
@SUBITUSINT #SUBITUSINT
+1 849-849-8576
+34 671454059
Guía para la elaboración de Programas de Protección Civil y Planes de Contingencias. Para Estados, Municipios y Delegaciones. MEXICO pdf Gratis

Enlace para DESCARGAR

SUBITUS International
@SUBITUSINT #SUBITUSINT
+1 849-849-8576
+34 671454059
martes, 2 de abril de 2019
The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition 2019 FREE pdf
 |
| The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition 2019 FREE pdf |
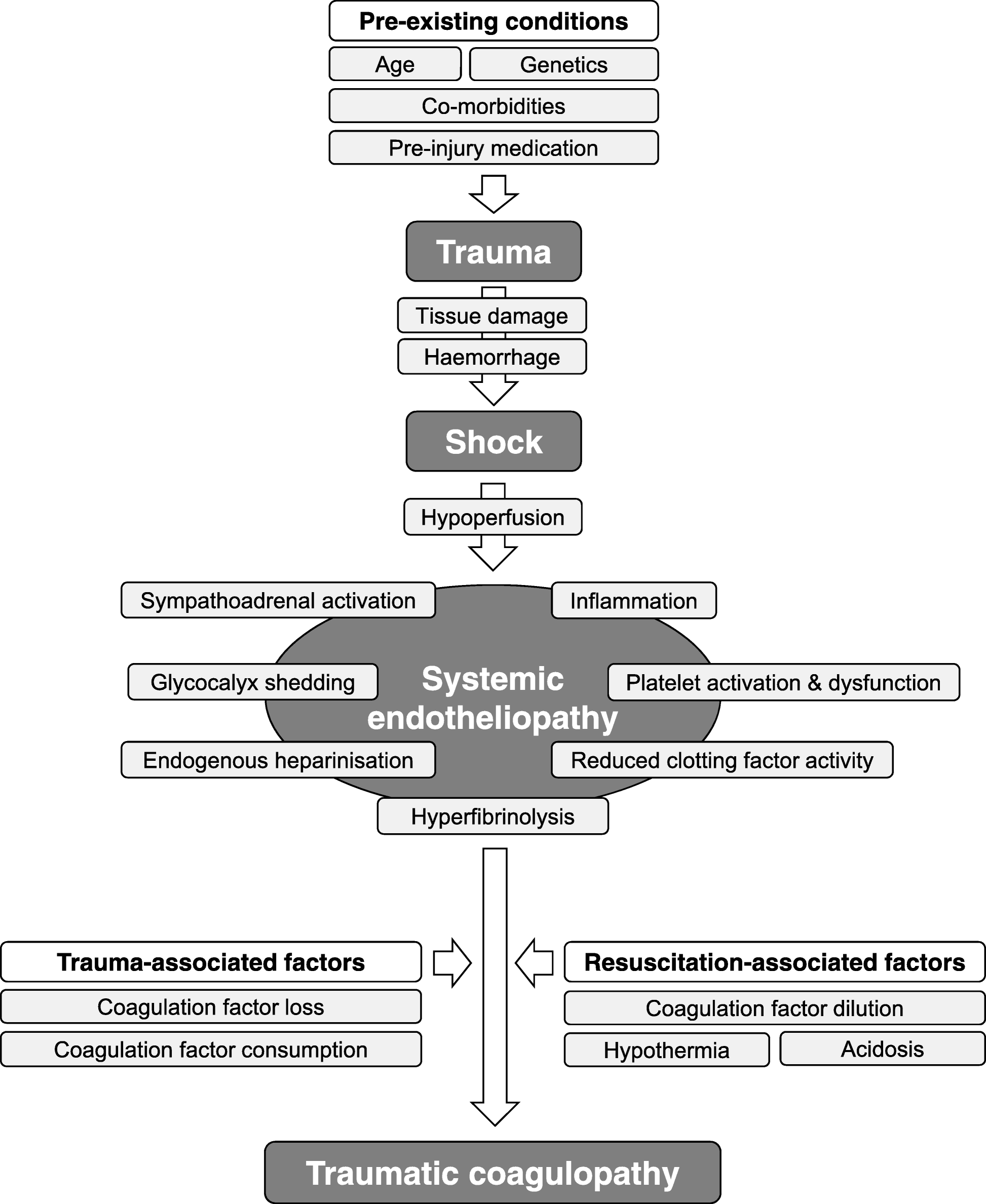
The appropriate management of trauma patients with massive bleeding and coagulopathy remains a major challenge in routine clinical practice. A multidisciplinary approach and adherence to evidence-based guidance are key to improving patient outcomes, which could now be shown in the first outcome studies.
DOWNLOAD free pdf
read full articule
Check if is updated

Fig. 2
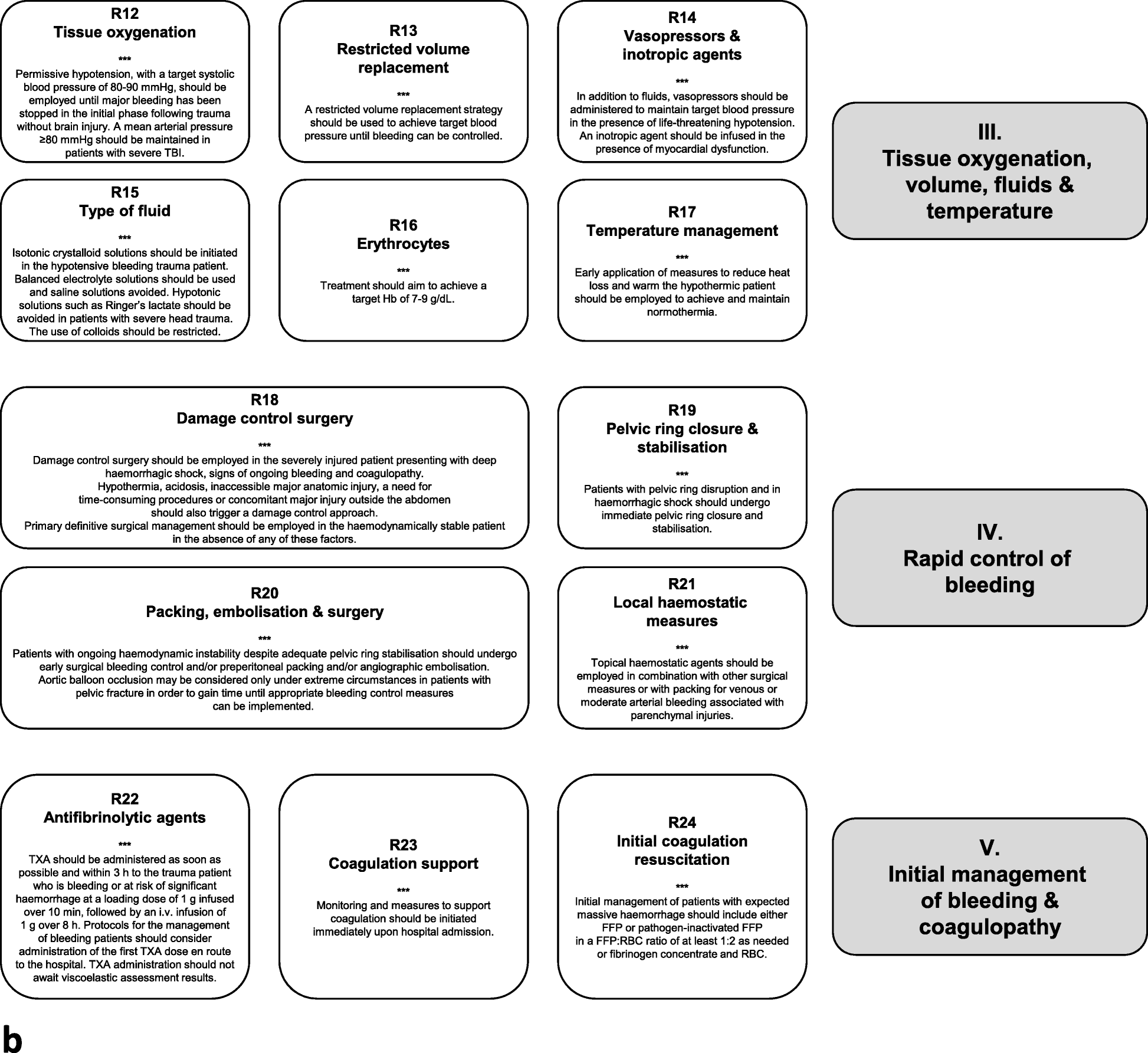
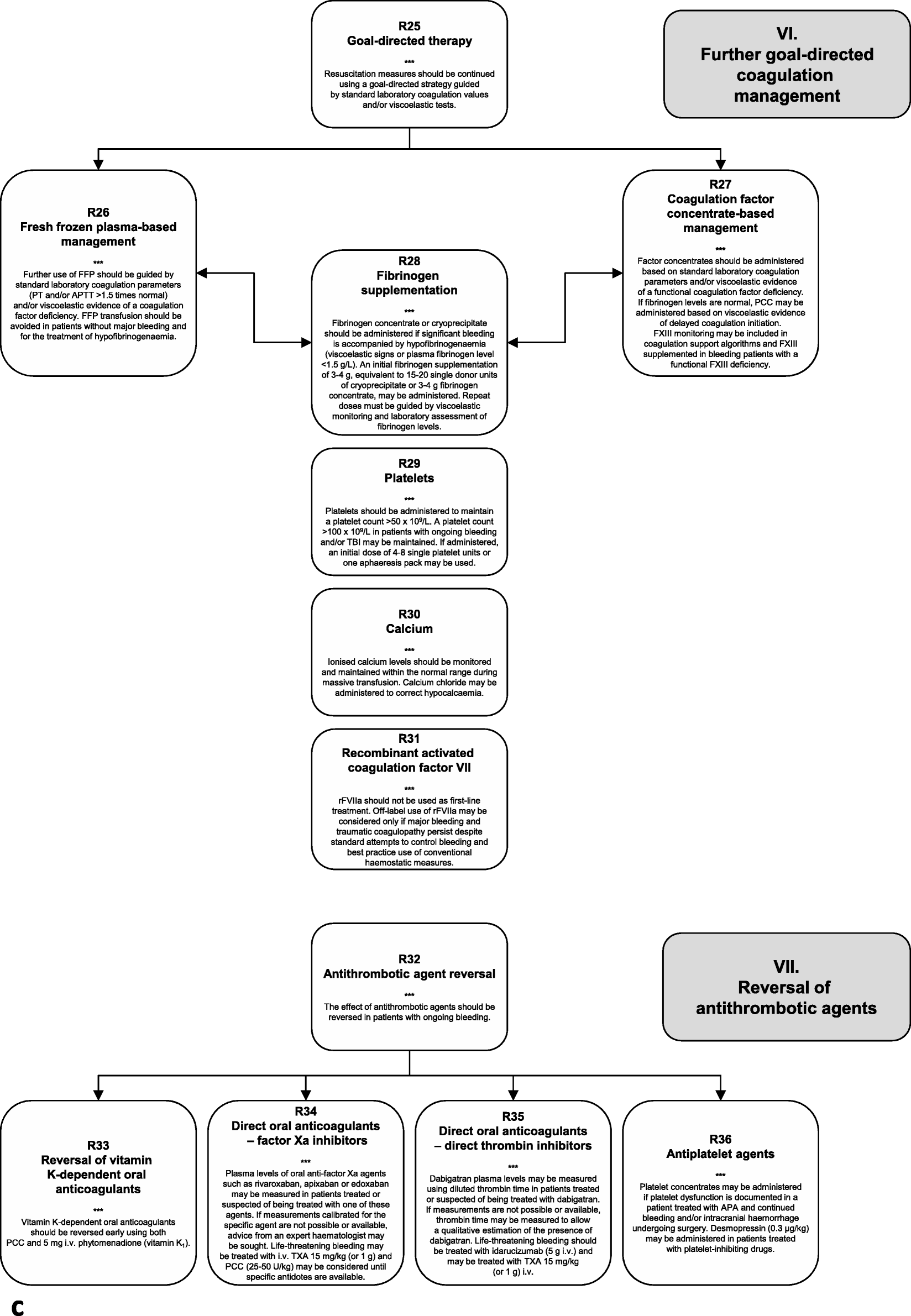
a Summary of treatment modalities for the bleeding trauma patients included in this guideline. CT, computed tomography; FAST, focused assessment with sonography in trauma; Hb, haemoglobin; PT, prothrombin time. b Summary of treatment modalities for the bleeding trauma patients included in this guideline. FFP, fresh frozen plasma; Hb, haemoglobin; RBC, red blood cells; TBI, traumatic brain injury; TXA, tranexamic acid. cSummary of treatment modalities for the bleeding trauma patients included in this guideline. APA, antiplatelet agent; APTT, activated partial thromboplastin time; FFP, fresh frozen plasma; FXIII, factor XIII; PCC, prothrombin complex concentrate; PT, prothrombin time; rFVIIa, recombinant activated coagulation factor VII; TBI, traumatic brain injury; TXA, tranexamic acid




SUBITUS International
@SUBITUSINT #SUBITUSINT
+1 849-849-8576
+34 671454059
domingo, 31 de marzo de 2019
VALORACION DEL PACIENTE POLITRAUMATIZADO SES ESPAÑA 2018 pdf
 |
Enlace para DESCARGAR pdf gratis
Mas documentos en pdf sobre TRAUMA en el siguiente enlace
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
| Escala de Coma de Glasgow http://emssolutionsint.blogspot.com/2011/12/glasgow-coma-scale-escala-de-coma-de.html |


SUBITUS International
@SUBITUSINT #SUBITUSINT
+1 849-849-8576
+34 671454059
lunes, 18 de marzo de 2019
Situational Awareness for First Responders. byJeremy Holder Following Managing Director at TacMed Australia

Original in LinkedIn
Over the last couple of months, I have noticed an increase in the number of incidents where Police Officers, especially Motorcycle Officers, have been injured in the line of duty. See a video HERE from Queensland Police where an officer is rammed by an offender and injured.
The video got me thinking as to how and what I would do if I was a First Responder rolling up to that scene to treat the officer or if I was responding to a similar high-threat incident. Note I am viewing this from a medical first response POV and not as a Law Enforcement POV.
Not just the medical treatment of the casualty but the whole scene and environment. It's dark, raining and there is a bad person somewhere who wants to hurt people.
What is your thought process? How would you approach this scene and not only treat the patient but the whole scene?
When responding to a trauma incident, I am a big fan of the MARCH mnemonic. MARCH is an amazing tool to use when assessing and treating a trauma casualty but what it lacks is the assessment of the environment or scene. This is where we place an “S” onto the front of MARCH for Security/Scene/Safety.
S- SCENE SAFETY/SECURITY
M- MASSIVE HAEMORRHAGE
A- AIRWAY
R- RESPIRATIONS
C- CIRCULATION
H- HEAD INJURY AND HYPOTHERMIA
The more commonly used DR(S)ABCDE primary survey is inappropriate for First Responders in a complex and dynamic environment as it implies that once you deem the scene safe from Danger, it will remain safe for the rest of your casualty treatment.
Not only do we need to ensure that the scene is initially safe enough to enter, or to provide security and/or neutralise the threat if you are a LEO, but we need to maintain situational awareness throughout the ongoing treatment of the casualty. To ensure this, when we train Police and other First Responders in any of our Tactical First Aid courses, we will get participants to go "heads up" between each part of the primary survey so they can maintain Situational Awareness and not become tunnel visioned on the casualty.
What is Situational Awareness (SA)? SA is the cognisance or awareness of what is happening around you. It not only includes who is around you but where you are and where you should be. Who or what is a threat to your health and safety.
In my opinion, Jason Bourne is the Grand Kung Fu master of Situational Awareness. Always reading his surroundings to get one step ahead of the next assassin's trying to knock him off.
“OBSERVE & ORIENTATE= SITUATIONAL AWARENESS”
For the more experienced First Responders reading this, we know SA is not something we can just read in a book or Linkedin article, and immediately become a Jedi Master in scene safety and situational awareness. Knowledge, education and experience will assist us in developing Situational Awareness.
An example of Situational Awareness (or lack of) is a job on the Ambulance where we attended a standard mental health call to a middle-aged male patient who is complaining of hearing the voice of the devil. I was working with a Trainee Paramedic who after accessing the house, walked up to the patient and knelt next to him, introduced themselves and preceded to ask the standard mental health questions in a non-threatening and sensitive demeanour.
The compassion and sincerity this young trainee showed were amazing but they focused solely on the patient and didn't have any SA. They had in fact, missed some key signs that had red-flagged this patient as a potential threat to both us and the patient. After walking into the house behind the trainee and orienting myself to the scene I was able to quickly identify the following :
- A large kitchen knife on the messy dining room table only a few meters from the patient (I’m not sure about you but I normally keep mine in the kitchen)
- An envelope on the coffee table that had the word “sorry” on the front
- The patient sounded agitated, had engorged neck veins and was clenching his right fist
Now thankfully nothing went wrong on this job and we were able to handle the situation safely and effectively but as you can imagine it could have gone very bad, very quickly.
Having the Situational Awareness mindset is imperative for First Responders. Don’t just tick that “scene safe” or "Danger" box and then put the scene/safety/security assessment away in the back of your mind. Constantly keep it in the front of your mind and maintain SA and thus your safety!
Stay safe, keep your head up and eyes open.
Jeremy Holder: Managing Director TacMed Australia
If you are interested in any first aid training for tactical, high-threat or complex environments you can lodge a training enquiry HERE.

Skype: drtolete
Facebook: @drramonreyesmd
LinkeIn https://es.linkedin.com/
LinkeIn https://es.linkedin.com/
Twitter: @DrtoleteMD
Instagram: https://www.instagram.com/
Instagram: https://www.instagram.com/

SUBITUS International
@SUBITUSINT #SUBITUSINT
https://web.facebook.com/
+1 849-849-8576
+34 671454059
subitusint@gmail.com
@SUBITUSINT #SUBITUSINT
https://web.facebook.com/
+1 849-849-8576
+34 671454059
subitusint@gmail.com
Suscribirse a:
Entradas (Atom)