



 | ||
Compilado by
CODIGO ICTUS MADRID. Atención a pacientes con ictus en la Comunidad de Madrid. pdf Gratis
emssolutionsint.blogspot.com/2018/07/codigo-ictus-madrid-atencion-pacientes.html Medidas de actuación en el ICTUS o ataque cerebral agudo. Servicio Andaluz de Salud
http://emssolutionsint.blogspot.com/2016/07/medidas-de-actuacion-en-el-ictus-o.html Prevención, identificación y actuación en el ICTUS. Tiempo es cerebro. Llama al 061 http://emssolutionsint.blogspot.com/2018/07/medidas-de-actuacion-en-el-ictus-o.html Guia Practica ICTUS
emssolutionsint.blogspot.com/2018/01/guia-practica-ictus.html Principios de los Cuidados del Accidente Cerebrovascular, ICTUS Isquemico emssolutionsint.blogspot.com/2011/04/cadena-de-supervivencia-por-ictus.html Guía de información al paciente con ICTUS "Guía de información al paciente con ICTUS"
emssolutionsint.blogspot.com/2016/07/guia-de-informacion-al-paciente-con.html Guía de información al paciente con ICTUS en formato pdf emssolutionsint.blogspot.com/2018/07/guia-de-informacion-al-paciente-con.html Prevención, identificación y actuación en el ICTUS. Tiempo es cerebro. Llama al 061 emssolutionsint.blogspot.com/2018/07/prevencion-identificacion-y-actuacion.html CODIGO ICTUS MADRID. Atención a pacientes con ictus en la Comunidad de Madrid. pdf Gratis
emssolutionsint.blogspot.com/2018/07/codigo-ictus-madrid-atencion-pacientes.html Guia de atencion al ICTUS. Servicio Canario de Salud. España PDF Gratis emssolutionsint.blogspot.com/2018/06/guia-de-atencion-al-ictus-servicio.html
Ambulancia Neuro-Protegida del Mundo. En el estadio Boca en Argentina
emssolutionsint.blogspot.com/2015/07/primer-estado-neuro-protegido-del-mundo.html
GUÍA DE TRATAMIENTO MULTIDISCIPLINAR EN EL ICTUS ISQUÉMICO AGUDO EN LA COMUNIDAD DE LA RIOJA PDF Gratis
Tratamiento de ictus isquémico agudo en pacientes con COVID-19  
Unas bacterias orales podrían ser las causantes de las embolias cerebrales 1 JUNIO, 2019 Un estudio finés ha demostrado que la embolia cerebral en pacientes que han sufrido un accidente cerebrovascular contiene ADN de patógenos orales, unas bacterias que provienen de los dientes y que son inofensivos, pero que cuando entran en circulación pueden causar, entre otras cosas, infecciones de las válvulas cardíacas, haciendo que el paciente sea más propenso a desarrollar coágulos en la sangre. El estudio, publicado en la revista americana Journal of American Heart Association, se basó en analizar los trombos que radiólogos neurointervencionales retiraron de 75 pacientes de accidente cerebrovascular como parte de una actuación en urgencias. Estas muestras fueron estudiadas duplicando el ADN bacteriano, mostrando que el 79% de ellos contenían ADN de bacterias que provenían de los dientes. Precisamente, el mismo grupo de investigación de este estudio ya había demostrado previamente que las mismas bacterias odontogénicas están presentes en las estenosis de las arterias coronarios de las pacientes que han muerto de forma repentina, en las aspiraciones de trombo y en la sangre arterial de los casos de infarto de miocardio, en los aneurismas cerebrales rotos y en los casos de aspiraciones de trombo en pacientes con trombosis arterial y venosa de miembros inferiores. Los resultados mostraron que una gran cantidad de ADN de “streptococcus viridans” (bacterias habituales en la boca) se encontró en los trombos cerebrales, muchos más de los había en las muestras de sangre de los mismos pacientes. Fuente: Infosalus MAS LIBROS MEDICINA Y SALUD https://www.facebook.com/pg/DrRamonReyesMD/photos/?tab=album&album_id=620883388254594 Dr. Ramon Reyes, MD
La pérdida de fuerza repentina en extremidades, la dificultad para hablar, para sonreír o coordinar movimientos acostumbran a ser los síntomas más evidentes de que una persona está sufriendo un accidente cerebrovascular. También se conoce como ictus, embolia o apoplejía.
En nuestro país, el ictus afecta cada año a unas 130.000 personas, de las cuales un 30% fallece y un 30% queda con algún tipo de discapacidad. Actualmente es la segunda causa de mortalidad en España, la primera en las mujeres.
Esta enfermedad es más frecuente a partir de los 55 años y su riesgo aumenta proporcionalmente con la edad, aunque también puede afectar a pacientes jóvenes e incluso a niños. DEFINICIÓN
Un accidente cerebrovascular o ictus es una enfermedad que afecta al cerebro por la disminución u obstrucción de la sangre que llega hasta él. Las neuronas (células nerviosas) al no llegarles sangre tampoco les llega oxígeno y dejan de funcionar.
Puede ser provocado por un coágulo que obstruye el paso de la sangre hacia el cerebro (ictus isquémico) o bien por una hemorragia por la rotura de un vaso cerebral (ictus hemorrágico). Aproximadamente el 85% de los ictus son isquémicos y el 15% hemorrágicos.
 SÍNTOMAS
La identificación inmediata de estos síntomas es crucial para la evolución del enfermo:
CONSEJOS PREVENCIÓN
La aparición del ictus se asocia a diferentes factores de riesgo, la mayoría de ellos evitables con una adecuada prevención. El control de los factores de riesgo es fundamental en la lucha contra esta patología. Toma nota de algunos consejos:
CONSEJOS ACTUACIÓN
Ante la presencia de alguno de los síntomas característicos, llama al 1-1-2 inmediatamente y sigue los consejos del personal sanitario. La rápida actuación de los Servicios de Emergencia es fundamental para la recuperación de lesiones en los pacientes que presentan un ictus.
  |
- Atención Primaria Basada en la Evidencia.
- http://www.ics.gencat.cat/3clics/main.php?page=GuiaPage&idGuia=599&idEsp=3
- Federación Española de Ictus. www.ictusfederacion.es
- Observatorio del Ictus. www.observatoriodelictus.com
- Grupo de Estudio de Enfermedades cerebrovasculares de la Sociedad Española de Neurologia. www.ictus.sen.es
- Federación Española de Daño Cerebral www.fedace.org
Referencias bibliográficas1 Benjamin EJ, Muntner P, Alonso A, et al, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019;139:e56-528. doi:10.1161/CIR.0000000000000659
2 National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-7. doi:10.1056/NEJM199512143332401
3 Hacke W, Kaste M, Bluhmki E, et al, ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J
Med 2008;359:1317-29. doi:10.1056/NEJMoa0804656
4 Goyal M, Menon BK, van Zwam WH, et al, HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016;387:1723-31. doi:10.1016/S0140-6736(16)00163-X
5 Albers GW, Marks MP, Kemp S, et al, DEFUSE 3 Investigators. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med 2018;378:708-18. doi:10.1056/NEJMoa1713973
6 Nogueira RG, Jadhav AP, Haussen DC, et al, DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med 2018;378:11-21. doi:10.1056/NEJMoa1706442
7 Emberson J, Lees KR, Lyden P, et al, Stroke Thrombolysis Trialists’ Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929-35. doi:10.1016/S0140-6736(14)60584-5
8 Fonarow GC, Zhao X, Smith EE, et al. Door-to-needle times for tissue plasminogen activator administration and clinical outcomes in acute ischemic stroke before and after a quality improvement initiative. JAMA 2014;311:1632-40. doi:10.1001/jama.2014.3203
9 Saver JL, Goyal M, van der Lugt A, et al, HERMES Collaborators. Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016;316:1279-88.doi:10.1001/jama.2016.13647
10 Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019;50:e344-418. doi:10.1161/STR.0000000000000211
11 Pierot L, Jayaraman MV, Szikora I, et al, Asian-Australian Federation of Interventional and Therapeutic Neuroradiology (AAFITN), Australianand New Zealand Society of Neuroradiology (ANZSNR), American Society of Neuroradiology (ASNR), Canadian Society of Neuroradiology (CSNR), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Japanese Society for NeuroEndovascular Therapy (JSNET), The French Society of Neuroradiology (SFNR) Ibero-Latin American Society of Diagnostic and Therapeutic Neuroradiology (SILAN), Society of NeuroInterventional Surgery (SNIS), Society of Vascular and Interventional Neurology (SVIN), World Stroke Organization (WSO), World Federation of Interventional Neuroradiology (WFITN). Standards of practice in acute ischemic stroke intervention: international recommendations. J Neurointerv Surg 2018;10:1121-6. doi:10.1136/neurintsurg-2018-014287
12 Adeoye O, Nyström KV, Yavagal DR, et al. Recommendations for the Establishment of Stroke Systems of Care: A 2019 Update. Stroke 2019;50:e187-210. doi:10.1161/STR.0000000000000173
13 Benoit JL, Khatri P, Adeoye OM, et al. Prehospital Triage of Acute Ischemic Stroke Patients to an Intravenous tPA-Ready versus Endovascular-Ready Hospital: A Decision Analysis. Prehosp Emerg Care 2018;22:722-33. doi:10.1080/10903127.2018.1465500
14 Froehler MT, Saver JL, Zaidat OO, et al, STRATIS Investigators. Interhospital Transfer Before Thrombectomy Is Associated With Delayed Treatment and Worse Outcome in the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke). Circulation 2017;136:2311-21.doi:10.1161/CIRCULATIONAHA.117.028920
15 Behrndtz A, Johnsen SP, Valentin JB, et al. TRIAGE-STROKE: Treatment strategy In Acute larGE vessel occlusion: Prioritize IV or endovascular treatment-A randomized trial. Int J Stroke 2019;1747493019869830. doi:10.1177/1747493019869830
16 Vidale S, Agostoni E. Prehospital stroke scales and large vessel occlusion: A systematic review. Acta Neurol Scand 2018;138:24-31.doi:10.1111/ane.12908
17 Kim JT, Chung PW, Starkman S, et al, FAST-MAG Trial (Field Administration of Stroke Therapy–Magnesium) Nurse-Coordinators and Investigators. Field Validation of the Los Angeles Motor Scale as a Tool for Paramedic Assessment of Stroke Severity. Stroke 2017;48:298-306. doi:10.1161/STROKEAHA.116.015247
18 Katz BS, McMullan JT, Sucharew H, Adeoye O, Broderick JP. Design and validation of a prehospital scale to predict stroke severity: Cincinnati Prehospital Stroke Severity Scale. Stroke 2015;46:1508-12. doi:10.1161/STROKEAHA.115.008804
19 Pérez de la Ossa N, Carrera D, Gorchs M, et al. Design and validation of a prehospital stroke scale to predict large arterial occlusion: the rapid arterial occlusion evaluation scale. Stroke 2014;45:87-91. doi:10.1161/STROKEAHA.113.003071
20 Teleb MS, Ver Hage A, Carter J, Jayaraman MV, McTaggart RA. Stroke vision, aphasia, neglect (VAN) assessment-a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. J Neurointerv Surg 2017;9:122-6. doi:10.1136/neurintsurg-2015-012131
21 Scheitz JF, Abdul-Rahim AH, MacIsaac RL, et al, SITS Scientific Committee. Clinical Selection Strategies to Identify Ischemic Stroke Patients With Large Anterior Vessel Occlusion: Results From SITS-ISTR (Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Registry). Stroke 2017;48:290-7. doi:10.1161/STROKEAHA.116.014431
22 Vidale S, Arnaboldi M, Frangi L, Longoni M, Monza G, Agostoni E. The Large ARtery Intracranial Occlusion Stroke Scale: A New Tool With High Accuracy in Predicting Large Vessel Occlusion. Front Neurol 2019;10:130. doi:10.3389/fneur.2019.00130
23 Calderon VJ, Kasturiarachi BM, Lin E, Bansal V, Zaidat OO. Review of the Mobile Stroke Unit Experience Worldwide. Interv Neurol 2018;7:347-58. doi:10.1159/000487334 24 Helwig SA, Ragoschke-Schumm A, Schwindling L, et al. Prehospital Stroke Management Optimized by Use of Clinical Scoring vs Mobile Stroke Unit for Triage of Patients With Stroke: A Randomized Clinical Trial. JAMA Neurol 2019. doi:10.1001/jamaneurol.2019.2829
25 Kepplinger J, Barlinn K, Deckert S, Scheibe M, Bodechtel U, Schmitt J. Safety and efficacy of thrombolysis in telestroke: A systematic review and meta-analysis. Neurology 2016;87:1344-51. doi:10.1212/WNL.0000000000003148
26 Zhang D, Shi L, Ido MS, et al. Impact of Participation in a Telestroke Network on Clinical Outcomes. Circ Cardiovasc Qual Outcomes 2019;12:e005147. doi:10.1161/CIRCOUTCOMES.118.005147
27 Ehrlich ME, Turner HL, Currie LJ, Wintermark M, Worrall BB, Southerland AM. Safety of Computed Tomographic Angiography in the Evaluation of Patients With Acute Stroke: A Single-Center Experience. Stroke 2016;47:2045-50. doi:10.1161/STROKEAHA.116.013973
28 Lima FO, Lev MH, Levy RA, et al. Functional contrast-enhanced CT for evaluation of acute ischemic stroke does not increase the risk of contrast-induced nephropathy. AJNR Am J Neuroradiol 2010;31:817-21. doi:10.3174/ajnr.A1927
29 Hopyan JJ, Gladstone DJ, Mallia G, et al. Renal safety of CT angiography and perfusion imaging in the emergency evaluation of acute stroke. AJNR Am J Neuroradiol 2008;29:1826-30. doi:10.3174/ajnr.A1257
30 Ang TE, Bivard A, Levi C, et al. Multi-modal CT in acute stroke: wait for a serum creatinine before giving intravenous contrast? No!Int J Stroke 2015;10:1014-7. doi:10.1111/ijs.12605
31 ACR–ASNR–SIR–SNIS Practice parameter for the performance of endovascular embolectomy and revascularization in acute stroke. 2018. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Acute-Stroke.pdf?la=en. 32 Ma H, Campbell BCV, Parsons MW, et al, EXTEND Investigators. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. N Engl J Med 2019;380:1795-803. doi:10.1056/NEJMoa1813046
33 Hacke W, Kaste M, Fieschi C, et al, The European Cooperative Acute Stroke Study (ECASS). Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. JAMA 1995;274:1017-25. doi:10.1001/jama.1995.03530130023023
34 Hacke W, Kaste M, Fieschi C, et al, Second European-Australasian Acute Stroke Study Investigators. Randomised double-blind placebocontrolled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998;352:1245-51. doi:10.1016/S0140-6736(98)08020-9
35 Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA 1999;282:2019-26. doi:10.1001/jama.282.21.2019
36 Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g) : results of a doubleblind, placebo-controlled, multicenter study. Thromblytic therapy in acute ischemic stroke study investigators. Stroke 2000;31:811-6. doi:10.1161/01.STR.31.4.811
37 Hacke W, Donnan G, Fieschi C, et al, AT LANTIS Trials Investigators, ECASS Trials Investigators, NINDS rt-PA Study Group Investigators. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004;363:768-74. doi:10.1016/S0140-6736(04)15692-4
38 Del Zoppo GJ, Saver JL, Jauch EC, Adams HPJrAmerican Heart Association Stroke Council. Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke 2009;40:2945-8. doi:10.1161/STROKEAHA.109.192535
39 Demaerschalk BM, Kleindorfer DO, Adeoye OM, et al, American Heart Association Stroke Council and Council on Epidemiology and Prevention. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2016;47:581-641. doi:10.1161/STR.0000000000000086
40 Albers GW, Thijs VN, Wechsler L, et al, DEFUSE Investigators. Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol 2006;60:508-17. doi:10.1002/ana.20976
41 Thomalla G, Cheng B, Ebinger M, et al, STIR and VISTA Imaging Investigators. DWI-FLAIR mismatch for the identification of patients with acute ischaemic stroke within 4·5 h of symptom onset (PRE-FLAIR): a multicentre observational study. Lancet Neurol 2011;10:978-86. doi:10.1016/S1474-4422(11)70192-2
42 Thomalla G, Simonsen CZ, Boutitie F, et al, WAKE-UP Investigators. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. N Engl J Med 2018;379:611-22. doi:10.1056/NEJMoa1804355
43 Campbell BCV, Ma H, Ringleb PA, et al, EXTEND, ECASS-4, and EPITHET Investigators. Extending thrombolysis to 4.5-9 h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data. Lancet 2019;394:139-47. doi:10.1016/S0140-6736(19)31053-0
44 Haley ECJr, Thompson JLP, Grotta JC, et al, Tenecteplase in Stroke Investigators. Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial. Stroke 2010;41:707-11. doi:10.1161/STROKEAHA.109.572040
45 Huang X, Cheripelli BK, Lloyd SM, et al. Alteplase versus tenecteplase for thrombolysis after ischaemic stroke (ATTEST): a phase 2, randomised, open-label, blinded endpoint study. Lancet Neurol 2015;14:368-76. doi:10.1016/S1474-4422(15)70017-7
46 Parsons M, Spratt N, Bivard A, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med 2012;366:1099-107. doi:10.1056/NEJMoa1109842
47 Logallo N, Novotny V, Assmus J, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol 2017;16:781-8. doi:10.1016/S1474-4422(17)30253-3
48 Campbell BCV, Mitchell PJ, Churilov L, et al, EXTEND-IA TNK Investigators. Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. N Engl J Med 2018;378:1573-82. doi:10.1056/
NEJMoa1716405
49 Campbell BC, Mitchell PJ, Churilov L, et al, EXTEND-IA TNK Investigators. Tenecteplase versus alteplase before endovascular thrombectomy (EXTEND-IA TNK): A multicenter, randomized, controlled study. Int J Stroke 2018;13:328-34. doi:10.1177/1747493017733935
50 Burgos AM, Saver JL. Evidence that Tenecteplase Is Noninferior to Alteplase for Acute Ischemic Stroke. Stroke 2019;50:2156-62. doi:10.1161/STROKEAHA.119.025080
51 Yaghi S, Willey JZ, Cucchiara B, et al, American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Quality of Care and Outcomes Research. Treatment and Outcome of Hemorrhagic Transformation After Intravenous Alteplase in Acute Ischemic Stroke: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2017;48:e343-61. doi:10.1161/STR.0000000000000152
52 Broderick JP, Palesch YY, Demchuk AM, et al, Interventional Management of Stroke (IMS) III Investigators. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med 2013;368:893-903. doi:10.1056/NEJMoa1214300
53 Kidwell CS, Jahan R, Gornbein J, et al, MR RESCUE Investigators. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med 2013;368:914-23. doi:10.1056/NEJMoa1212793
54 Ciccone A, Valvassori L, Nichelatti M, et al, SYNTHESIS Expansion Investigators. Endovascular treatment for acute ischemic stroke. N Engl J Med 2013;368:904-13. doi:10.1056/NEJMoa1213701
55 Alberts MJ, Shang T, Magadan A. Endovascular Therapy for Acute Ischemic Stroke: Dawn of a New Era. JAMA Neurol 2015;72:1101-3. doi:10.1001/jamaneurol.2015.1743
56 Berkhemer OA, Fransen PS, Beumer D, et al, MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11-20. doi:10.1056/NEJMoa1411587
57 Goyal M, Demchuk AM, Menon BK, et al, ESCAPE Trial Investigators. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015;372:1019-30. doi:10.1056/NEJMoa1414905
58 Campbell BC, Mitchell PJ, Kleinig TJ, et al, EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015;372:1009-18. doi:10.1056/NEJMoa1414792
59 Saver JL, Goyal M, Bonafe A, et al, SWIFT PRIME Investigators. Stentretriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015;372:2285-95. doi:10.1056/NEJMoa1415061 60 Jovin TG, Chamorro A, Cobo E, et al, REVASCAT Trial Investigators. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 2015;372:2296-306. doi:10.1056/NEJMoa1503780 61 Mocco J, Zaidat OO, von Kummer R, et al, THERAPY Trial Investigators*. Aspiration Thrombectomy After Intravenous Alteplase Versus Intravenous Alteplase Alone. Stroke 2016;47:2331-8. doi:10.1161/STROKEAHA.116.013372
62 Bracard S, Ducrocq X, Mas JL, et al, THRACE investigators. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol 2016;15:1138-47. doi:10.1016/S1474-4422(16)30177-6
63 Muir KW, Ford GA, Messow CM, et al, PISTE Investigators. Endovascular therapy for acute ischaemic stroke: the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) randomised, controlled trial. J Neurol Neurosurg Psychiatry 2017;88:38-44. doi:10.1136/jnnp-2016-314117
64 Almekhlafi MA, Hill MD, Roos YM, et al. Stroke Laterality Did Not Modify Outcomes in the HERMES Meta-Analysis of Individual Patient Data of 7 Trials. Stroke 2019;50:2118-24. doi:10.1161/STROKEAHA.118.023102
65 McMeekin P, White P, James MA, Price CI, Flynn D, Ford GA. Estimating the number of UK stroke patients eligible for endovascular thrombectomy. Eur Stroke J 2017;2:319-26. doi:10.1177/2396987317733343
66 Jadhav AP, Desai SM, Kenmuir CL, et al. Eligibility for Endovascular Trial Enrollment in the 6- to 24-Hour Time Window: Analysis of a Single Comprehensive Stroke Center. Stroke 2018;49:1015-7. doi:10.1161/STROKEAHA.117.020273
67 Campbell BC, Hill MD, Rubiera M, et al. Safety and Efficacy of Solitaire Stent Thrombectomy: Individual Patient Data Meta-Analysis of Randomized Trials. Stroke 2016;47:798-806. doi:10.1161/STROKEAHA.115.012360
68 Zaidat OO, Yoo AJ, Khatri P, et al, Cerebral Angiographic Revascularization Grading (CARG) Collaborators, STIR Revascularization working group, STIR Thrombolysis in Cerebral Infarction (TICI) Task Force. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke 2013;44:2650-63. doi:10.1161/STROKEAHA.113.001972
69 Saver JL, Jahan R, Levy EI, et al, SWIFT Trialists. Solitaire Flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, noninferiority trial. Lancet 2012;380:1241-9. doi:10.1016/S0140-6736(12)61384-1
70 Broussalis E, Trinka E, Hitzl W, Wallner A, Chroust V, Killer-Oberpfalzer M. Comparison of stent-retriever devices versus the Merci retriever for endovascular treatment of acute stroke. AJNR Am J Neuroradiol 2013;34:366-72. doi:10.3174/ajnr.A3195
71 Deng L, Qiu S, Wang L, Li Y, Wang D, Liu M. Comparison of Four Food and Drug Administration-Approved Mechanical Thrombectomy Devices for Acute Ischemic Stroke: A Network Meta-Analysis. World Neurosurg 2019;127:e49-57. doi:10.1016/j.wneu.2019.02.011
72 Zaidat OO, Bozorgchami H, Ribó M, et al. Primary Results of the Multicenter ARISE II Study (Analysis of Revascularization in Ischemic Stroke With EmboTrap). Stroke 2018;49:1107-15. doi:10.1161/STROKEAHA.117.020125
73 Jindal G, Serulle Y, Miller T, et al. Stent retrieval thrombectomy in acute stoke is facilitated by the concurrent use of intracranial aspiration catheters. J Neurointerv Surg 2017;9:944-7. doi:10.1136/neurintsurg-2016-012581
74 Turk AS, Turner R, Spiotta A, et al. Comparison of endovascular treatment approaches for acute ischemic stroke: cost effectiveness, technical success, and clinical outcomes. J Neurointerv Surg 2015;7:666-70. doi:10.1136/neurintsurg-2014-011282
75 Lapergue B, Blanc R, Gory B, et al, ASTER Trial Investigators. Effect of Endovascular Contact Aspiration vs Stent Retriever on Revascularization in Patients With Acute Ischemic Stroke and Large Vessel Occlusion: The ASTER Randomized Clinical Trial. JAMA 2017;318:443-52. doi:10.1001/jama.2017.9644
76 Gory B, Lapergue B, Blanc R, et al, ASTER Trial Investigators. Contact Aspiration Versus Stent Retriever in Patients With Acute Ischemic Stroke With M2 Occlusion in the ASTER Randomized Trial (Contact Aspiration Versus Stent Retriever for Successful Revascularization). Stroke 2018;49:461-4. doi:10.1161/STROKEAHA.117.019598
77 Turk AS3rd, Siddiqui A, Fifi JT, et al. spiration thrombectomy versus stent retriever thrombectomy as first-line approach for large vessel occlusion (COMPASS): a multicentre, randomised, open label, blinded outcome, non-inferiority trial. Lancet 2019;393:998-1008. doi:10.1016/S0140-6736(19)30297-1
78 Wan TF, Xu R, Zhao ZA, Lv Y, Chen HS, Liu L. Outcomes of general anesthesia versus conscious sedation for Stroke undergoing endovascular treatment: a meta-analysis. BMC Anesthesiol 2019;19:69. doi:10.1186/s12871-019-0741-7
79 Abou-Chebl A, Lin R, Hussain MS, et al. Conscious sedation versus general anesthesia during endovascular therapy for acute anterior circulation stroke: preliminary results from a retrospective, multicenter study. Stroke 2010;41:1175-9. doi:10.1161/STROKEAHA.109.574129
80 Jumaa MA, Zhang F, Ruiz-Ares G, et al. Comparison of safety and clinical and radiographic outcomes in endovascular acute stroke therapy for proximal middle cerebral artery occlusion with intubation and general anesthesia versus the nonintubated state. Stroke 2010;41:1180-4. doi:10.1161/STROKEAHA.109.574194
81 John N, Mitchell P, Dowling R, Yan B. Is general anaesthesia preferible to conscious sedation in the treatment of acute ischaemic stroke with intra-arterial mechanical thrombectomy? A review of the literature. Neuroradiology 2013;55:93-100. doi:10.1007/s00234-012-1084-y
82 Brinjikji W, Murad MH, Rabinstein AA, Cloft HJ, Lanzino G, Kallmes DF. Conscious sedation versus general anesthesia during endovascular acute ischemic stroke treatment: a systematic review and meta-analysis. AJNR Am J Neuroradiol 2015;36:525-9. doi:10.3174/ajnr.A4159
83 Just C, Rizek P, Tryphonopoulos P, Pelz D, Arango M. Outcomes of General Anesthesia and Conscious Sedation in Endovascular Treatment for Stroke. Can J Neurol Sci 2016;43:655-8. doi:10.1017/cjn.2016.256
84 Löwhagen Hendén P, Rentzos A, Karlsson JE, et al. General Anesthesia Versus Conscious Sedation for Endovascular Treatment of Acute Ischemic Stroke: The AnStroke Trial (Anesthesia During Stroke). Stroke 2017;48:1601-7. doi:10.1161/STROKEAHA.117.016554
85 Schönenberger S, Uhlmann L, Hacke W, et al. Effect of Conscious Sedation vs General Anesthesia on Early Neurological Improvement Among Patients With Ischemic Stroke Undergoing Endovascular Thrombectomy: A Randomized Clinical Trial. JAMA 2016;316:1986-
96. doi:10.1001/jama.2016.16623
86 Simonsen CZ, Yoo AJ, Sørensen LH, et al. Effect of General Anesthesia and Conscious Sedation During Endovascular Therapy on Infarct Growth and Clinical Outcomes in Acute Ischemic Stroke: A Randomized Clinical Trial. JAMA Neurol 2018;75:470-7. doi:10.1001/jamaneurol.2017.4474
87 Schönenberger S, Hendén PL, Simonsen CZ, et al. Association of General Anesthesia vs Procedural Sedation With Functional Outcome Among Patients With Acute Ischemic Stroke Undergoing Thrombectomy: A Systematic Review and Meta-analysis. JAMA 2019;322:1283-93. doi:10.1001/jama.2019.11455
88 Powers CJ, Dornbos D3rd, Mlynash M, et al. Thrombectomy with Conscious Sedation Compared with General Anesthesia: A DEFUSE 3 Analysis. AJNR Am J Neuroradiol 2019;40:1001-5. doi:10.3174/ajnr. A6059
89 Campbell BCV, van Zwam WH, Goyal M, et al, HERMES collaborators. Effect of general anaesthesia on functional outcome in patients with anterior circulation ischaemic stroke having endovascular thrombectomy versus standard care: a meta-analysis of individual patient data. Lancet Neurol 2018;17:47-53. doi:10.1016/S1474-4422(17)30407-6
90 Bath PM, Scutt P, Anderson CS, et al, RIGHT-2 Investigators. Prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2): an ambulance-based, randomised, sham-controlled, blinded, phase 3 trial. Lancet 2019;393:1009-20. doi:10.1016/S0140-6736(19)30194-1
91 Lee M, Ovbiagele B, Hong KS, et al. Effect of Blood Pressure Lowering in Early Ischemic Stroke: Meta-Analysis. Stroke 2015;46:1883-9. doi:10.1161/STROKEAHA.115.009552
92 Anderson CS, Huang Y, Lindley RI, et al, ENCHANTED Investigators and Coordinators. Intensive blood pressure reduction with intravenous thrombolysis therapy for acute ischaemic stroke (ENCHANTED): an international, randomised, open-label, blinded-endpoint, phase 3 trial. Lancet 2019;393:877-88. doi:10.1016/S0140-6736(19)30038-8
93 Goyal N, Tsivgoulis G, Pandhi A, et al. Blood pressure levels post mechanical thrombectomy and outcomes in large vessel occlusion strokes. Neurology 2017;89:540-7. doi:10.1212/WNL.0000000000004184
94 Mistry EA, Mayer SA, Khatri P. Blood Pressure Management after Mechanical Thrombectomy for Acute Ischemic Stroke: A Survey of the StrokeNet Sites. J Stroke Cerebrovasc Dis 2018;27:2474-8. doi:10.1016/j.jstrokecerebrovasdis.2018.05.003
95 Wojner-Alexander AW, Garami Z, Chernyshev OY, Alexandrov AV. Heads down: flat positioning improves blood flow velocity in acute ischemic stroke. Neurology 2005;64:1354-7. doi:10.1212/01. WNL.0000158284.41705.A5
96 Hargroves D, Tallis R, Pomeroy V, Bhalla A. The influence of positioning upon cerebral oxygenation after acute stroke: a pilot study. Age Ageing 2008;37:581-5. doi:10.1093/ageing/afn143
97 Olavarría VV, Arima H, Anderson CS, et al. Head position and cerebral blood flow velocity in acute ischemic stroke: a systematic review and meta-analysis. Cerebrovasc Dis 2014;37:401-8. doi:10.1159/000362533
98 Truijen J, Rasmussen LS, Kim YS, et al. Cerebral autoregulatory performance and the cerebrovascular response to head-of-bed positioning in acute ischaemic stroke. Eur J Neurol 2018;25:1365-e117. doi:10.1111/ene.13737
99 Olavarría VV, Lavados PM, Muñoz-Venturelli P, et al. Flat-head positioning increases cerebral blood flow in anterior circulation acute ischemic stroke. A cluster randomized phase IIb trial. Int J
Stroke 2018;13:600-11. doi:10.1177/1747493017711943
100 Anderson CS, Arima H, Lavados P, et al, HeadPoST Investigators and Coordinators. Cluster-Randomized, Crossover Trial of Head Positioning in Acute Stroke. N Engl J Med 2017;376:2437-47. doi:10.1056/NEJMoa1615715
101 Alexandrov AW, Tsivgoulis G, Hill MD, et al. HeadPoST: Rightly positioned, or flat out wrong?Neurology 2018;90:885-9. doi:10.1212/WNL.0000000000005481
102 Johnston KC, Bruno A, Pauls Q, et al, Neurological Emergencies Treatment Trials Network and the SHINE Trial Investigators. Intensive vs Standard Treatment of Hyperglycemia and Functional Outcome in Patients With Acute Ischemic Stroke: The SHINE Randomized Clinical Trial. JAMA 2019;322:326-35. doi:10.1001/jama.2019.9346
103 Roffe C, Nevatte T, Sim J, et al, Stroke Oxygen Study Investigators and the Stroke OxygenStudy Collaborative Group. Effect of Routine Low-Dose Oxygen Supplementation on Death and Disability in Adults With Acute Stroke: The Stroke Oxygen Study Randomized Clinical Trial. JAMA 2017;318:1125-35. doi:10.1001/jama.2017.11463
104 CAST (Chinese Acute Stroke Trial) Collaborative Group. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997;349:1641-9. doi:10.1016/S0140-6736(97)04010-5
105 International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349:1569-81. doi:10.1016/S0140-6736(97)04011-7
106 Wang Y, Wang Y, Zhao X, et al, CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-9. doi:10.1056/NEJMoa1215340
107 Johnston SC, Easton JD, Farrant M, et al, Clinical Research Collaboration, Neurological Emergencies Treatment Trials Network, and the POINT Investigators. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. N Engl J Med 2018;379:215-25. doi:10.1056/NEJMoa1800410
108 Prasad K, Siemieniuk R, Hao Q, et al. Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline. BMJ 2018;363:k5130. doi:10.1136/bmj.k5130
109 Campbell BCV, Majoie CBLM, Albers GW, et al, HERMES collaborators. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patientlevel data. Lancet Neurol 2019;18:46-55. doi:10.1016/S1474-4422(18)30314-4
110 Román LS, Menon BK, Blasco J, et al, HERMES collaborators. Imaging features and safety and efficacy of endovascular stroke treatment: a meta-analysis of individual patient-level data. Lancet Neurol 2018;17:895-904. doi:10.1016/S1474-4422(18)30242-4
111 Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. lberta Stroke Programme Early CT Score. Lancet 2000;355:1670-4. doi:10.1016/S0140- 736(00)02237-6
112 Nagel S, Bouslama M, Krause LU, et al. Mechanical Thrombectomy in Patients With Milder Strokes and Large Vessel Occlusions. Stroke 2018;49:2391-7. doi:10.1161/STROKEAHA.118.021106
113 Sarraj A, Hassan A, Savitz SI, et al. Endovascular Thrombectomy for Mild Strokes: How Low Should We Go?Stroke 2018;49:2398-405. doi:10.1161/STROKEAHA.118.022114
114 Brehm A, Tsogkas I, Maier IL, et al. One-Stop Management with Perfusion for Transfer Patients with Stroke due to a Large-Vessel Occlusion: Feasibility and Effects on In-Hospital Times. AJNR Am J Neuroradiol 2019;40:1330-4. doi:10.3174/ajnr.A6129
115 Psychogios MN, Behme D, Schregel K, et al. One-Stop Management of Acute Stroke Patients: Minimizing Door-to-Reperfusion Times. Stroke 2017;48:3152-5. doi:10.1161/STROKEAHA.117.018077
116 Boncoraglio GB, Ranieri M, Bersano A, Parati EA, Del Giovane C. Stem cell transplantation for ischemic stroke. Cochrane Database Syst Rev 2019;5:CD007231.
117 Patel RAG, McMullen PW. Neuroprotection in the Treatment of Acute Ischemic Stroke. Prog Cardiovasc Dis 2017;59:542-8. doi:10.1016/j.pcad.2017.04.005
118 Griauzde J, Ravindra VM, Chaudhary N, Gemmete JJ, Pandey AS. Neuroprotection for ischemic stroke in the endovascular era: A brief report on the future of intra-arterial therapy. J Clin Neurosci 2019;69:289-91. doi:10.1016/j.jocn.2019.08.001
119 Boulanger JM, Lindsay MP, Gubitz G, et al. Canadian Stroke Best Practice Recommendations for Acute Stroke Management: Prehospital, Emergency Department, and Acute Inpatient Stroke Care, 6th Edition, Update 2018. Int J Stroke 2018;13:949-84. doi:10.1177/1747493018786616
1 Benjamin EJ, Muntner P, Alonso A, et al, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019;139:e56-528. doi:10.1161/CIR.0000000000000659
2 National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-7. doi:10.1056/NEJM199512143332401
3 Hacke W, Kaste M, Bluhmki E, et al, ECASS Investigators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J
Med 2008;359:1317-29. doi:10.1056/NEJMoa0804656
4 Goyal M, Menon BK, van Zwam WH, et al, HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016;387:1723-31. doi:10.1016/S0140-6736(16)00163-X
5 Albers GW, Marks MP, Kemp S, et al, DEFUSE 3 Investigators. Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging. N Engl J Med 2018;378:708-18. doi:10.1056/NEJMoa1713973
6 Nogueira RG, Jadhav AP, Haussen DC, et al, DAWN Trial Investigators. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N Engl J Med 2018;378:11-21. doi:10.1056/NEJMoa1706442
7 Emberson J, Lees KR, Lyden P, et al, Stroke Thrombolysis Trialists’ Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929-35. doi:10.1016/S0140-6736(14)60584-5
8 Fonarow GC, Zhao X, Smith EE, et al. Door-to-needle times for tissue plasminogen activator administration and clinical outcomes in acute ischemic stroke before and after a quality improvement initiative. JAMA 2014;311:1632-40. doi:10.1001/jama.2014.3203
9 Saver JL, Goyal M, van der Lugt A, et al, HERMES Collaborators. Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. JAMA 2016;316:1279-88.doi:10.1001/jama.2016.13647
10 Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019;50:e344-418. doi:10.1161/STR.0000000000000211
11 Pierot L, Jayaraman MV, Szikora I, et al, Asian-Australian Federation of Interventional and Therapeutic Neuroradiology (AAFITN), Australianand New Zealand Society of Neuroradiology (ANZSNR), American Society of Neuroradiology (ASNR), Canadian Society of Neuroradiology (CSNR), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Japanese Society for NeuroEndovascular Therapy (JSNET), The French Society of Neuroradiology (SFNR) Ibero-Latin American Society of Diagnostic and Therapeutic Neuroradiology (SILAN), Society of NeuroInterventional Surgery (SNIS), Society of Vascular and Interventional Neurology (SVIN), World Stroke Organization (WSO), World Federation of Interventional Neuroradiology (WFITN). Standards of practice in acute ischemic stroke intervention: international recommendations. J Neurointerv Surg 2018;10:1121-6. doi:10.1136/neurintsurg-2018-014287
12 Adeoye O, Nyström KV, Yavagal DR, et al. Recommendations for the Establishment of Stroke Systems of Care: A 2019 Update. Stroke 2019;50:e187-210. doi:10.1161/STR.0000000000000173
13 Benoit JL, Khatri P, Adeoye OM, et al. Prehospital Triage of Acute Ischemic Stroke Patients to an Intravenous tPA-Ready versus Endovascular-Ready Hospital: A Decision Analysis. Prehosp Emerg Care 2018;22:722-33. doi:10.1080/10903127.2018.1465500
14 Froehler MT, Saver JL, Zaidat OO, et al, STRATIS Investigators. Interhospital Transfer Before Thrombectomy Is Associated With Delayed Treatment and Worse Outcome in the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke). Circulation 2017;136:2311-21.doi:10.1161/CIRCULATIONAHA.117.028920
15 Behrndtz A, Johnsen SP, Valentin JB, et al. TRIAGE-STROKE: Treatment strategy In Acute larGE vessel occlusion: Prioritize IV or endovascular treatment-A randomized trial. Int J Stroke 2019;1747493019869830. doi:10.1177/1747493019869830
16 Vidale S, Agostoni E. Prehospital stroke scales and large vessel occlusion: A systematic review. Acta Neurol Scand 2018;138:24-31.doi:10.1111/ane.12908
17 Kim JT, Chung PW, Starkman S, et al, FAST-MAG Trial (Field Administration of Stroke Therapy–Magnesium) Nurse-Coordinators and Investigators. Field Validation of the Los Angeles Motor Scale as a Tool for Paramedic Assessment of Stroke Severity. Stroke 2017;48:298-306. doi:10.1161/STROKEAHA.116.015247
18 Katz BS, McMullan JT, Sucharew H, Adeoye O, Broderick JP. Design and validation of a prehospital scale to predict stroke severity: Cincinnati Prehospital Stroke Severity Scale. Stroke 2015;46:1508-12. doi:10.1161/STROKEAHA.115.008804
19 Pérez de la Ossa N, Carrera D, Gorchs M, et al. Design and validation of a prehospital stroke scale to predict large arterial occlusion: the rapid arterial occlusion evaluation scale. Stroke 2014;45:87-91. doi:10.1161/STROKEAHA.113.003071
20 Teleb MS, Ver Hage A, Carter J, Jayaraman MV, McTaggart RA. Stroke vision, aphasia, neglect (VAN) assessment-a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. J Neurointerv Surg 2017;9:122-6. doi:10.1136/neurintsurg-2015-012131
21 Scheitz JF, Abdul-Rahim AH, MacIsaac RL, et al, SITS Scientific Committee. Clinical Selection Strategies to Identify Ischemic Stroke Patients With Large Anterior Vessel Occlusion: Results From SITS-ISTR (Safe Implementation of Thrombolysis in Stroke International Stroke Thrombolysis Registry). Stroke 2017;48:290-7. doi:10.1161/STROKEAHA.116.014431
22 Vidale S, Arnaboldi M, Frangi L, Longoni M, Monza G, Agostoni E. The Large ARtery Intracranial Occlusion Stroke Scale: A New Tool With High Accuracy in Predicting Large Vessel Occlusion. Front Neurol 2019;10:130. doi:10.3389/fneur.2019.00130
23 Calderon VJ, Kasturiarachi BM, Lin E, Bansal V, Zaidat OO. Review of the Mobile Stroke Unit Experience Worldwide. Interv Neurol 2018;7:347-58. doi:10.1159/000487334 24 Helwig SA, Ragoschke-Schumm A, Schwindling L, et al. Prehospital Stroke Management Optimized by Use of Clinical Scoring vs Mobile Stroke Unit for Triage of Patients With Stroke: A Randomized Clinical Trial. JAMA Neurol 2019. doi:10.1001/jamaneurol.2019.2829
25 Kepplinger J, Barlinn K, Deckert S, Scheibe M, Bodechtel U, Schmitt J. Safety and efficacy of thrombolysis in telestroke: A systematic review and meta-analysis. Neurology 2016;87:1344-51. doi:10.1212/WNL.0000000000003148
26 Zhang D, Shi L, Ido MS, et al. Impact of Participation in a Telestroke Network on Clinical Outcomes. Circ Cardiovasc Qual Outcomes 2019;12:e005147. doi:10.1161/CIRCOUTCOMES.118.005147
27 Ehrlich ME, Turner HL, Currie LJ, Wintermark M, Worrall BB, Southerland AM. Safety of Computed Tomographic Angiography in the Evaluation of Patients With Acute Stroke: A Single-Center Experience. Stroke 2016;47:2045-50. doi:10.1161/STROKEAHA.116.013973
28 Lima FO, Lev MH, Levy RA, et al. Functional contrast-enhanced CT for evaluation of acute ischemic stroke does not increase the risk of contrast-induced nephropathy. AJNR Am J Neuroradiol 2010;31:817-21. doi:10.3174/ajnr.A1927
29 Hopyan JJ, Gladstone DJ, Mallia G, et al. Renal safety of CT angiography and perfusion imaging in the emergency evaluation of acute stroke. AJNR Am J Neuroradiol 2008;29:1826-30. doi:10.3174/ajnr.A1257
30 Ang TE, Bivard A, Levi C, et al. Multi-modal CT in acute stroke: wait for a serum creatinine before giving intravenous contrast? No!Int J Stroke 2015;10:1014-7. doi:10.1111/ijs.12605
31 ACR–ASNR–SIR–SNIS Practice parameter for the performance of endovascular embolectomy and revascularization in acute stroke. 2018. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Acute-Stroke.pdf?la=en. 32 Ma H, Campbell BCV, Parsons MW, et al, EXTEND Investigators. Thrombolysis Guided by Perfusion Imaging up to 9 Hours after Onset of Stroke. N Engl J Med 2019;380:1795-803. doi:10.1056/NEJMoa1813046
33 Hacke W, Kaste M, Fieschi C, et al, The European Cooperative Acute Stroke Study (ECASS). Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. JAMA 1995;274:1017-25. doi:10.1001/jama.1995.03530130023023
34 Hacke W, Kaste M, Fieschi C, et al, Second European-Australasian Acute Stroke Study Investigators. Randomised double-blind placebocontrolled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998;352:1245-51. doi:10.1016/S0140-6736(98)08020-9
35 Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. The ATLANTIS Study: a randomized controlled trial. Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke. JAMA 1999;282:2019-26. doi:10.1001/jama.282.21.2019
36 Clark WM, Albers GW, Madden KP, Hamilton S. The rtPA (alteplase) 0- to 6-hour acute stroke trial, part A (A0276g) : results of a doubleblind, placebo-controlled, multicenter study. Thromblytic therapy in acute ischemic stroke study investigators. Stroke 2000;31:811-6. doi:10.1161/01.STR.31.4.811
37 Hacke W, Donnan G, Fieschi C, et al, AT LANTIS Trials Investigators, ECASS Trials Investigators, NINDS rt-PA Study Group Investigators. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004;363:768-74. doi:10.1016/S0140-6736(04)15692-4
38 Del Zoppo GJ, Saver JL, Jauch EC, Adams HPJrAmerican Heart Association Stroke Council. Expansion of the time window for treatment of acute ischemic stroke with intravenous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Stroke 2009;40:2945-8. doi:10.1161/STROKEAHA.109.192535
39 Demaerschalk BM, Kleindorfer DO, Adeoye OM, et al, American Heart Association Stroke Council and Council on Epidemiology and Prevention. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2016;47:581-641. doi:10.1161/STR.0000000000000086
40 Albers GW, Thijs VN, Wechsler L, et al, DEFUSE Investigators. Magnetic resonance imaging profiles predict clinical response to early reperfusion: the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) study. Ann Neurol 2006;60:508-17. doi:10.1002/ana.20976
41 Thomalla G, Cheng B, Ebinger M, et al, STIR and VISTA Imaging Investigators. DWI-FLAIR mismatch for the identification of patients with acute ischaemic stroke within 4·5 h of symptom onset (PRE-FLAIR): a multicentre observational study. Lancet Neurol 2011;10:978-86. doi:10.1016/S1474-4422(11)70192-2
42 Thomalla G, Simonsen CZ, Boutitie F, et al, WAKE-UP Investigators. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. N Engl J Med 2018;379:611-22. doi:10.1056/NEJMoa1804355
43 Campbell BCV, Ma H, Ringleb PA, et al, EXTEND, ECASS-4, and EPITHET Investigators. Extending thrombolysis to 4.5-9 h and wake-up stroke using perfusion imaging: a systematic review and meta-analysis of individual patient data. Lancet 2019;394:139-47. doi:10.1016/S0140-6736(19)31053-0
44 Haley ECJr, Thompson JLP, Grotta JC, et al, Tenecteplase in Stroke Investigators. Phase IIB/III trial of tenecteplase in acute ischemic stroke: results of a prematurely terminated randomized clinical trial. Stroke 2010;41:707-11. doi:10.1161/STROKEAHA.109.572040
45 Huang X, Cheripelli BK, Lloyd SM, et al. Alteplase versus tenecteplase for thrombolysis after ischaemic stroke (ATTEST): a phase 2, randomised, open-label, blinded endpoint study. Lancet Neurol 2015;14:368-76. doi:10.1016/S1474-4422(15)70017-7
46 Parsons M, Spratt N, Bivard A, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med 2012;366:1099-107. doi:10.1056/NEJMoa1109842
47 Logallo N, Novotny V, Assmus J, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol 2017;16:781-8. doi:10.1016/S1474-4422(17)30253-3
48 Campbell BCV, Mitchell PJ, Churilov L, et al, EXTEND-IA TNK Investigators. Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. N Engl J Med 2018;378:1573-82. doi:10.1056/
NEJMoa1716405
49 Campbell BC, Mitchell PJ, Churilov L, et al, EXTEND-IA TNK Investigators. Tenecteplase versus alteplase before endovascular thrombectomy (EXTEND-IA TNK): A multicenter, randomized, controlled study. Int J Stroke 2018;13:328-34. doi:10.1177/1747493017733935
50 Burgos AM, Saver JL. Evidence that Tenecteplase Is Noninferior to Alteplase for Acute Ischemic Stroke. Stroke 2019;50:2156-62. doi:10.1161/STROKEAHA.119.025080
51 Yaghi S, Willey JZ, Cucchiara B, et al, American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Quality of Care and Outcomes Research. Treatment and Outcome of Hemorrhagic Transformation After Intravenous Alteplase in Acute Ischemic Stroke: A Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2017;48:e343-61. doi:10.1161/STR.0000000000000152
52 Broderick JP, Palesch YY, Demchuk AM, et al, Interventional Management of Stroke (IMS) III Investigators. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med 2013;368:893-903. doi:10.1056/NEJMoa1214300
53 Kidwell CS, Jahan R, Gornbein J, et al, MR RESCUE Investigators. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med 2013;368:914-23. doi:10.1056/NEJMoa1212793
54 Ciccone A, Valvassori L, Nichelatti M, et al, SYNTHESIS Expansion Investigators. Endovascular treatment for acute ischemic stroke. N Engl J Med 2013;368:904-13. doi:10.1056/NEJMoa1213701
55 Alberts MJ, Shang T, Magadan A. Endovascular Therapy for Acute Ischemic Stroke: Dawn of a New Era. JAMA Neurol 2015;72:1101-3. doi:10.1001/jamaneurol.2015.1743
56 Berkhemer OA, Fransen PS, Beumer D, et al, MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11-20. doi:10.1056/NEJMoa1411587
57 Goyal M, Demchuk AM, Menon BK, et al, ESCAPE Trial Investigators. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 2015;372:1019-30. doi:10.1056/NEJMoa1414905
58 Campbell BC, Mitchell PJ, Kleinig TJ, et al, EXTEND-IA Investigators. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med 2015;372:1009-18. doi:10.1056/NEJMoa1414792
59 Saver JL, Goyal M, Bonafe A, et al, SWIFT PRIME Investigators. Stentretriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 2015;372:2285-95. doi:10.1056/NEJMoa1415061 60 Jovin TG, Chamorro A, Cobo E, et al, REVASCAT Trial Investigators. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 2015;372:2296-306. doi:10.1056/NEJMoa1503780 61 Mocco J, Zaidat OO, von Kummer R, et al, THERAPY Trial Investigators*. Aspiration Thrombectomy After Intravenous Alteplase Versus Intravenous Alteplase Alone. Stroke 2016;47:2331-8. doi:10.1161/STROKEAHA.116.013372
62 Bracard S, Ducrocq X, Mas JL, et al, THRACE investigators. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol 2016;15:1138-47. doi:10.1016/S1474-4422(16)30177-6
63 Muir KW, Ford GA, Messow CM, et al, PISTE Investigators. Endovascular therapy for acute ischaemic stroke: the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) randomised, controlled trial. J Neurol Neurosurg Psychiatry 2017;88:38-44. doi:10.1136/jnnp-2016-314117
64 Almekhlafi MA, Hill MD, Roos YM, et al. Stroke Laterality Did Not Modify Outcomes in the HERMES Meta-Analysis of Individual Patient Data of 7 Trials. Stroke 2019;50:2118-24. doi:10.1161/STROKEAHA.118.023102
65 McMeekin P, White P, James MA, Price CI, Flynn D, Ford GA. Estimating the number of UK stroke patients eligible for endovascular thrombectomy. Eur Stroke J 2017;2:319-26. doi:10.1177/2396987317733343
66 Jadhav AP, Desai SM, Kenmuir CL, et al. Eligibility for Endovascular Trial Enrollment in the 6- to 24-Hour Time Window: Analysis of a Single Comprehensive Stroke Center. Stroke 2018;49:1015-7. doi:10.1161/STROKEAHA.117.020273
67 Campbell BC, Hill MD, Rubiera M, et al. Safety and Efficacy of Solitaire Stent Thrombectomy: Individual Patient Data Meta-Analysis of Randomized Trials. Stroke 2016;47:798-806. doi:10.1161/STROKEAHA.115.012360
68 Zaidat OO, Yoo AJ, Khatri P, et al, Cerebral Angiographic Revascularization Grading (CARG) Collaborators, STIR Revascularization working group, STIR Thrombolysis in Cerebral Infarction (TICI) Task Force. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke 2013;44:2650-63. doi:10.1161/STROKEAHA.113.001972
69 Saver JL, Jahan R, Levy EI, et al, SWIFT Trialists. Solitaire Flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, noninferiority trial. Lancet 2012;380:1241-9. doi:10.1016/S0140-6736(12)61384-1
70 Broussalis E, Trinka E, Hitzl W, Wallner A, Chroust V, Killer-Oberpfalzer M. Comparison of stent-retriever devices versus the Merci retriever for endovascular treatment of acute stroke. AJNR Am J Neuroradiol 2013;34:366-72. doi:10.3174/ajnr.A3195
71 Deng L, Qiu S, Wang L, Li Y, Wang D, Liu M. Comparison of Four Food and Drug Administration-Approved Mechanical Thrombectomy Devices for Acute Ischemic Stroke: A Network Meta-Analysis. World Neurosurg 2019;127:e49-57. doi:10.1016/j.wneu.2019.02.011
72 Zaidat OO, Bozorgchami H, Ribó M, et al. Primary Results of the Multicenter ARISE II Study (Analysis of Revascularization in Ischemic Stroke With EmboTrap). Stroke 2018;49:1107-15. doi:10.1161/STROKEAHA.117.020125
73 Jindal G, Serulle Y, Miller T, et al. Stent retrieval thrombectomy in acute stoke is facilitated by the concurrent use of intracranial aspiration catheters. J Neurointerv Surg 2017;9:944-7. doi:10.1136/neurintsurg-2016-012581
74 Turk AS, Turner R, Spiotta A, et al. Comparison of endovascular treatment approaches for acute ischemic stroke: cost effectiveness, technical success, and clinical outcomes. J Neurointerv Surg 2015;7:666-70. doi:10.1136/neurintsurg-2014-011282
75 Lapergue B, Blanc R, Gory B, et al, ASTER Trial Investigators. Effect of Endovascular Contact Aspiration vs Stent Retriever on Revascularization in Patients With Acute Ischemic Stroke and Large Vessel Occlusion: The ASTER Randomized Clinical Trial. JAMA 2017;318:443-52. doi:10.1001/jama.2017.9644
76 Gory B, Lapergue B, Blanc R, et al, ASTER Trial Investigators. Contact Aspiration Versus Stent Retriever in Patients With Acute Ischemic Stroke With M2 Occlusion in the ASTER Randomized Trial (Contact Aspiration Versus Stent Retriever for Successful Revascularization). Stroke 2018;49:461-4. doi:10.1161/STROKEAHA.117.019598
77 Turk AS3rd, Siddiqui A, Fifi JT, et al. spiration thrombectomy versus stent retriever thrombectomy as first-line approach for large vessel occlusion (COMPASS): a multicentre, randomised, open label, blinded outcome, non-inferiority trial. Lancet 2019;393:998-1008. doi:10.1016/S0140-6736(19)30297-1
78 Wan TF, Xu R, Zhao ZA, Lv Y, Chen HS, Liu L. Outcomes of general anesthesia versus conscious sedation for Stroke undergoing endovascular treatment: a meta-analysis. BMC Anesthesiol 2019;19:69. doi:10.1186/s12871-019-0741-7
79 Abou-Chebl A, Lin R, Hussain MS, et al. Conscious sedation versus general anesthesia during endovascular therapy for acute anterior circulation stroke: preliminary results from a retrospective, multicenter study. Stroke 2010;41:1175-9. doi:10.1161/STROKEAHA.109.574129
80 Jumaa MA, Zhang F, Ruiz-Ares G, et al. Comparison of safety and clinical and radiographic outcomes in endovascular acute stroke therapy for proximal middle cerebral artery occlusion with intubation and general anesthesia versus the nonintubated state. Stroke 2010;41:1180-4. doi:10.1161/STROKEAHA.109.574194
81 John N, Mitchell P, Dowling R, Yan B. Is general anaesthesia preferible to conscious sedation in the treatment of acute ischaemic stroke with intra-arterial mechanical thrombectomy? A review of the literature. Neuroradiology 2013;55:93-100. doi:10.1007/s00234-012-1084-y
82 Brinjikji W, Murad MH, Rabinstein AA, Cloft HJ, Lanzino G, Kallmes DF. Conscious sedation versus general anesthesia during endovascular acute ischemic stroke treatment: a systematic review and meta-analysis. AJNR Am J Neuroradiol 2015;36:525-9. doi:10.3174/ajnr.A4159
83 Just C, Rizek P, Tryphonopoulos P, Pelz D, Arango M. Outcomes of General Anesthesia and Conscious Sedation in Endovascular Treatment for Stroke. Can J Neurol Sci 2016;43:655-8. doi:10.1017/cjn.2016.256
84 Löwhagen Hendén P, Rentzos A, Karlsson JE, et al. General Anesthesia Versus Conscious Sedation for Endovascular Treatment of Acute Ischemic Stroke: The AnStroke Trial (Anesthesia During Stroke). Stroke 2017;48:1601-7. doi:10.1161/STROKEAHA.117.016554
85 Schönenberger S, Uhlmann L, Hacke W, et al. Effect of Conscious Sedation vs General Anesthesia on Early Neurological Improvement Among Patients With Ischemic Stroke Undergoing Endovascular Thrombectomy: A Randomized Clinical Trial. JAMA 2016;316:1986-
96. doi:10.1001/jama.2016.16623
86 Simonsen CZ, Yoo AJ, Sørensen LH, et al. Effect of General Anesthesia and Conscious Sedation During Endovascular Therapy on Infarct Growth and Clinical Outcomes in Acute Ischemic Stroke: A Randomized Clinical Trial. JAMA Neurol 2018;75:470-7. doi:10.1001/jamaneurol.2017.4474
87 Schönenberger S, Hendén PL, Simonsen CZ, et al. Association of General Anesthesia vs Procedural Sedation With Functional Outcome Among Patients With Acute Ischemic Stroke Undergoing Thrombectomy: A Systematic Review and Meta-analysis. JAMA 2019;322:1283-93. doi:10.1001/jama.2019.11455
88 Powers CJ, Dornbos D3rd, Mlynash M, et al. Thrombectomy with Conscious Sedation Compared with General Anesthesia: A DEFUSE 3 Analysis. AJNR Am J Neuroradiol 2019;40:1001-5. doi:10.3174/ajnr. A6059
89 Campbell BCV, van Zwam WH, Goyal M, et al, HERMES collaborators. Effect of general anaesthesia on functional outcome in patients with anterior circulation ischaemic stroke having endovascular thrombectomy versus standard care: a meta-analysis of individual patient data. Lancet Neurol 2018;17:47-53. doi:10.1016/S1474-4422(17)30407-6
90 Bath PM, Scutt P, Anderson CS, et al, RIGHT-2 Investigators. Prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2): an ambulance-based, randomised, sham-controlled, blinded, phase 3 trial. Lancet 2019;393:1009-20. doi:10.1016/S0140-6736(19)30194-1
91 Lee M, Ovbiagele B, Hong KS, et al. Effect of Blood Pressure Lowering in Early Ischemic Stroke: Meta-Analysis. Stroke 2015;46:1883-9. doi:10.1161/STROKEAHA.115.009552
92 Anderson CS, Huang Y, Lindley RI, et al, ENCHANTED Investigators and Coordinators. Intensive blood pressure reduction with intravenous thrombolysis therapy for acute ischaemic stroke (ENCHANTED): an international, randomised, open-label, blinded-endpoint, phase 3 trial. Lancet 2019;393:877-88. doi:10.1016/S0140-6736(19)30038-8
93 Goyal N, Tsivgoulis G, Pandhi A, et al. Blood pressure levels post mechanical thrombectomy and outcomes in large vessel occlusion strokes. Neurology 2017;89:540-7. doi:10.1212/WNL.0000000000004184
94 Mistry EA, Mayer SA, Khatri P. Blood Pressure Management after Mechanical Thrombectomy for Acute Ischemic Stroke: A Survey of the StrokeNet Sites. J Stroke Cerebrovasc Dis 2018;27:2474-8. doi:10.1016/j.jstrokecerebrovasdis.2018.05.003
95 Wojner-Alexander AW, Garami Z, Chernyshev OY, Alexandrov AV. Heads down: flat positioning improves blood flow velocity in acute ischemic stroke. Neurology 2005;64:1354-7. doi:10.1212/01. WNL.0000158284.41705.A5
96 Hargroves D, Tallis R, Pomeroy V, Bhalla A. The influence of positioning upon cerebral oxygenation after acute stroke: a pilot study. Age Ageing 2008;37:581-5. doi:10.1093/ageing/afn143
97 Olavarría VV, Arima H, Anderson CS, et al. Head position and cerebral blood flow velocity in acute ischemic stroke: a systematic review and meta-analysis. Cerebrovasc Dis 2014;37:401-8. doi:10.1159/000362533
98 Truijen J, Rasmussen LS, Kim YS, et al. Cerebral autoregulatory performance and the cerebrovascular response to head-of-bed positioning in acute ischaemic stroke. Eur J Neurol 2018;25:1365-e117. doi:10.1111/ene.13737
99 Olavarría VV, Lavados PM, Muñoz-Venturelli P, et al. Flat-head positioning increases cerebral blood flow in anterior circulation acute ischemic stroke. A cluster randomized phase IIb trial. Int J
Stroke 2018;13:600-11. doi:10.1177/1747493017711943
100 Anderson CS, Arima H, Lavados P, et al, HeadPoST Investigators and Coordinators. Cluster-Randomized, Crossover Trial of Head Positioning in Acute Stroke. N Engl J Med 2017;376:2437-47. doi:10.1056/NEJMoa1615715
101 Alexandrov AW, Tsivgoulis G, Hill MD, et al. HeadPoST: Rightly positioned, or flat out wrong?Neurology 2018;90:885-9. doi:10.1212/WNL.0000000000005481
102 Johnston KC, Bruno A, Pauls Q, et al, Neurological Emergencies Treatment Trials Network and the SHINE Trial Investigators. Intensive vs Standard Treatment of Hyperglycemia and Functional Outcome in Patients With Acute Ischemic Stroke: The SHINE Randomized Clinical Trial. JAMA 2019;322:326-35. doi:10.1001/jama.2019.9346
103 Roffe C, Nevatte T, Sim J, et al, Stroke Oxygen Study Investigators and the Stroke OxygenStudy Collaborative Group. Effect of Routine Low-Dose Oxygen Supplementation on Death and Disability in Adults With Acute Stroke: The Stroke Oxygen Study Randomized Clinical Trial. JAMA 2017;318:1125-35. doi:10.1001/jama.2017.11463
104 CAST (Chinese Acute Stroke Trial) Collaborative Group. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997;349:1641-9. doi:10.1016/S0140-6736(97)04010-5
105 International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349:1569-81. doi:10.1016/S0140-6736(97)04011-7
106 Wang Y, Wang Y, Zhao X, et al, CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-9. doi:10.1056/NEJMoa1215340
107 Johnston SC, Easton JD, Farrant M, et al, Clinical Research Collaboration, Neurological Emergencies Treatment Trials Network, and the POINT Investigators. Clopidogrel and Aspirin in Acute Ischemic Stroke and High-Risk TIA. N Engl J Med 2018;379:215-25. doi:10.1056/NEJMoa1800410
108 Prasad K, Siemieniuk R, Hao Q, et al. Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline. BMJ 2018;363:k5130. doi:10.1136/bmj.k5130
109 Campbell BCV, Majoie CBLM, Albers GW, et al, HERMES collaborators. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patientlevel data. Lancet Neurol 2019;18:46-55. doi:10.1016/S1474-4422(18)30314-4
110 Román LS, Menon BK, Blasco J, et al, HERMES collaborators. Imaging features and safety and efficacy of endovascular stroke treatment: a meta-analysis of individual patient-level data. Lancet Neurol 2018;17:895-904. doi:10.1016/S1474-4422(18)30242-4
111 Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. lberta Stroke Programme Early CT Score. Lancet 2000;355:1670-4. doi:10.1016/S0140- 736(00)02237-6
112 Nagel S, Bouslama M, Krause LU, et al. Mechanical Thrombectomy in Patients With Milder Strokes and Large Vessel Occlusions. Stroke 2018;49:2391-7. doi:10.1161/STROKEAHA.118.021106
113 Sarraj A, Hassan A, Savitz SI, et al. Endovascular Thrombectomy for Mild Strokes: How Low Should We Go?Stroke 2018;49:2398-405. doi:10.1161/STROKEAHA.118.022114
114 Brehm A, Tsogkas I, Maier IL, et al. One-Stop Management with Perfusion for Transfer Patients with Stroke due to a Large-Vessel Occlusion: Feasibility and Effects on In-Hospital Times. AJNR Am J Neuroradiol 2019;40:1330-4. doi:10.3174/ajnr.A6129
115 Psychogios MN, Behme D, Schregel K, et al. One-Stop Management of Acute Stroke Patients: Minimizing Door-to-Reperfusion Times. Stroke 2017;48:3152-5. doi:10.1161/STROKEAHA.117.018077
116 Boncoraglio GB, Ranieri M, Bersano A, Parati EA, Del Giovane C. Stem cell transplantation for ischemic stroke. Cochrane Database Syst Rev 2019;5:CD007231.
117 Patel RAG, McMullen PW. Neuroprotection in the Treatment of Acute Ischemic Stroke. Prog Cardiovasc Dis 2017;59:542-8. doi:10.1016/j.pcad.2017.04.005
118 Griauzde J, Ravindra VM, Chaudhary N, Gemmete JJ, Pandey AS. Neuroprotection for ischemic stroke in the endovascular era: A brief report on the future of intra-arterial therapy. J Clin Neurosci 2019;69:289-91. doi:10.1016/j.jocn.2019.08.001
119 Boulanger JM, Lindsay MP, Gubitz G, et al. Canadian Stroke Best Practice Recommendations for Acute Stroke Management: Prehospital, Emergency Department, and Acute Inpatient Stroke Care, 6th Edition, Update 2018. Int J Stroke 2018;13:949-84. doi:10.1177/1747493018786616
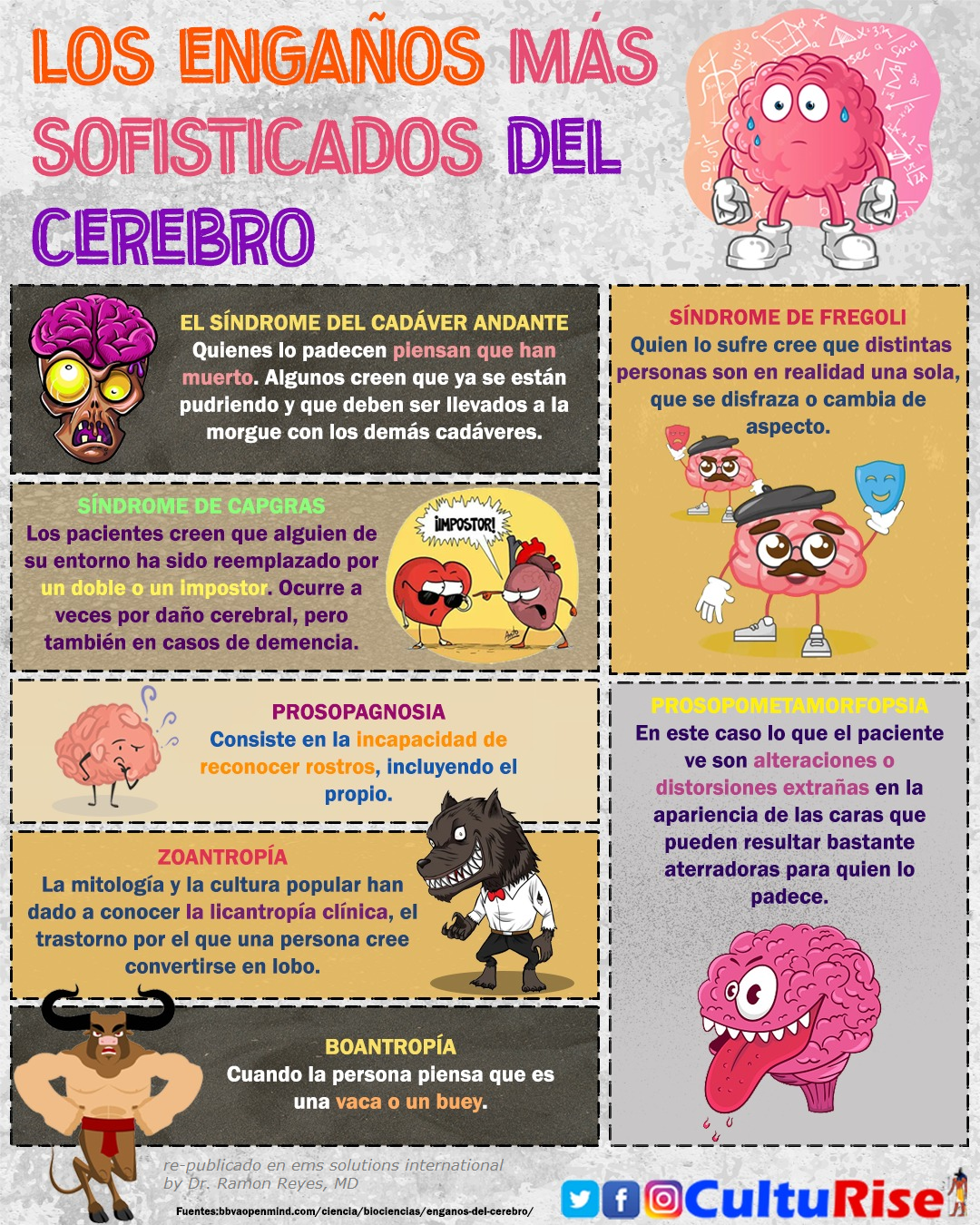 |
| LOS ENGAÑOS MAS SOFISTICADOS DEL CEREBRO by culturise |
No hay comentarios:
Publicar un comentario