




MEDEVAC CASEVAC TACEVAC
German air force's A400M planes to have intensive care stations
 |
💉😷 #Covid19 🦠 by @DrRamonReyesMD 🧪 🥼 🧬 🩺 TODO SOBRE LAS #VACUNAS #YoMeVacuno |
MEDEVAC "HISTORY AND TRIBUTE". Video by TACMED "Tactical Medicine" España http://emssolutionsint.blogspot.com/2017/03/medevac-history-and-tribute-video.html
PREPARACIÓN DEL PACIENTE PARA EVACUACIONES AÉREAS. Transporte Aeromedico http://emssolutionsint.blogspot.com/2013/07/preparacion-del-paciente-para.html
NATO ROLE Support "Role" or "Echelon. Military Hospitals. HOSPITALES DE CAMPAÑA OTAN-ESPAÑA http://emssolutionsint.blogspot.com/2015/11/nato-role-support-role-or-echelon.html
MAS LIBROS MEDICINA Y SALUD https://www.facebook.com/pg/DrRamonReyesMD/photos/?tab=album&album_id=620883388254594
Dr. Ramon Reyes, MD
Fuerza Aerea alemana adapta uno de sus A400M como Unidad de Ciuidados Intensivos Movil para sus MEDEVAC
https://www.defensa.com/otan-y-europa/fuerza-aerea-alemana-adapta-uno-a400m-como-uvi-movil






Todos Nuestros VIDEOS en YouTube https://www.youtube.com/c/RamonReyes2015


H 135 AIRBUS



TACTICAL EMERGENCY CASUALTY CARE TECC by C-TECC

MEDEVAC
MEDEVAC + CASEVAC =TACEVAC
La evacuación médica o MEDEVAC es un sistema de traslado de pacientes desde una ubicación remota hasta un hospital especializado, por lo general en el medio militar.
CASEVAC (casualty evacuation) se refiere a la evacuación utilizando cualquier medio de transporte, generalmente con una limitada o nula capacidad de brindar este cuidado médico mientras se traslada al paciente, y es utilizado cuando no hay tiempo para esperar a un MEDEVAC, o cuando éste se ve imposibilitado de acceder a la zona de rescate. El CASEVAC también es ampliamente utilizado debido a que muchos rescates se efectúan en zonas "rojas" y el fuego enemigo podría causar daños al equipo y/o personal médico.
La evacuación médica o MEDEVAC es un sistema de traslado de pacientes desde una ubicación remota hasta un hospital especializado, por lo general en el medio militar. El término MEDEVAC se aplica generalmente a un vehículo aéreo, a un avión, o a un helicóptero usado como ambulancia, a veces llamada una "ambulancia aérea". Esto permite el transporte rápido de las personas seriamente lesionadas, particularmente pacientes traumatizados, desde la escena de un accidente hasta un hospital especializado.
El término MEDEVAC puede ser mal interpretado, pues puede no clarificar si se está refiriendo a un transporte por tierra o por aire, por lo que siempre se debe especificar el método de evacuación durante la comunicación con los hospitales.
La técnica tiene sus inicios en los años 20, a partir del establecimiento en Australia de un sistema aéreo de socorro civil en el interior remoto y semi-árido de Australia, ya fuera para trasladar enfermos o heridos al hospital o para acercar la ayuda médica hasta lugares inhóspitos. Los helicópteros irrumpieron en el medio militar a finales de la Segunda Guerra Mundial, pero su empleo no se hizo habitual por parte del Ejército de los Estados Unidos para el transporte de heridos hasta la Guerra de Corea. Se establecieron hospitales quirúrgicos móviles justo detrás de las líneas de combate, que permitían que los soldados heridos recibieran tratamiento médico después de un corto vuelo en helicóptero. Esta táctica militar, generalizada ya en la Guerra de Vietnam, fue popularizada en la serie televisiva M*A*S*H de los años 70.
En la terminología militar norteamericana, se distingue a menudo por la evacuación de bajas. En este contexto, se refiere al traslado asistido de un paciente, bien sea desde el punto de la lesión a una instalación médica, o bien entre los diversos niveles de asistencia médica. Un vehículo de evacuación médica está por consiguiente, dotado con material de primeros auxilios a bordo, así como con personal médico entrenado como parte de la tripulación. El vehículo está marcado con la Cruz Roja (o con la Media Luna Roja), y como tal, cubierto por la convención de Ginebra, que protege teóricamente al vehículo de ataques de cualquiera de los bandos en conflicto, y solamente autoriza a la tripulación de vuelo a portar armas personales, no así armas de guerra.
En este sentido, un MEDEVAC se refiere a la evacuación por razones médicas desde la zona de combate, suceso o accidente, o un punto de extracción, hacia la base militar general o hacia un centro médico o incluso a una zona más segura, o entre los distintos niveles de asistencia al soldado y siempre contando con asistencia médica "en ruta" (on-route care), mientras que un CASEVAC (casualty evacuation) se refiere a la evacuación utilizando cualquier medio de transporte, generalmente con una limitada o nula capacidad de brindar este cuidado médico mientras se traslada al paciente, y es utilizado cuando no hay tiempo para esperar a un MEDEVAC, o cuando éste se ve imposibilitado de acceder a la zona de rescate. El CASEVAC también es ampliamente utilizado debido a que muchos rescates se efectúan en zonas "rojas" y el fuego enemigo podría causar daños al equipo y/o personal médico.
En terminología militar australiana, un MEDEVAC se refiere a la evacuación por razones médicas de una sección, tropa o pelotón, mientras que un CASEVAC se aplica a la evacuación de una sola persona.
El término 'evacuación aeromédica' o AEROVAC también se utiliza para hablar del transporte de pacientes desde un centro asistencial médico hasta otro con un nivel más alto de cuidados o a una instalación hospitalaria fija o en el caso del combate, a un ambiente más seguro; pero el vehículo siempre debe contar con capacidad para cuidados médicos especiales durante el transporte (como el uso de los ventiladores mecánicos, monitorización, etc).

Modern EMS practices have their roots in Vietnam medical rescues |
Medevac mission, Balad Air Base, Iraq
US Air Force Expeditionary Aeromedical Evacuation Squadron members monitor patients during a C-17 aero-medical evacuation mission from Balad Air Base, Iraq, to Ramstein Air Base, Germany. The Boeing (formerly McDonnell Douglas) C-17 Globemaster III is a large American airlifter manufactured by Boeing Integrated Defense Systems, and operated by the United States Air Force, British Royal Air Force, the Royal Australian Air Force, and the Canadian Forces.[3] NATO and Qatar will also acquire the airlifter.
The C-17 Globemaster III is capable of rapid strategic delivery of troops and all types of cargo to main operating bases or directly to forward bases in the deployment area. It is also capable of performing tactical airlift, medical evacuation and airdrop missions. The C-17 takes its name from two previous United States cargo aircraft, the C-74 Globemaster and the C-124 Globemaster II.
Specifications (C-17:) General characteristics Crew: 3: 2 pilots, 1 loadmaster Capacity: 102 troops or 36 litter and 54 ambulatory patients Payload: 170,900 lb (77,519 kg) of cargo distributed at max over 18 463L master pallets or a mix of palletized cargo and vehicles Length: 174 ft (53 m) Wingspan: 169.8 ft (51.75 m) Height: 55.1 ft (16.8 m) Wing area: 3,800 ft² (353 m²) Empty weight: 282,500 lb (128,100 kg) Max takeoff weight: 585,000 lb (265,350 kg) Powerplant: 4× Pratt & Whitney F117-PW-100 turbofans, 40,440 lbf (180 kN) each Fuel capacity: 35,546 US gal (134,556 L) Performance Cruise speed: Mach 0.76 (450 knots, 515 mph, 830 km/h) Range: 2,420 nmi[74] (2,785 mi, 4,482 km) Service ceiling 45,000 ft (13,716 m) Max wing loading: 150 lb/ft² (750 kg/m²) Minimum thrust/weight: 0.277
|

The first written record of the term "air ambulance" is in Jules Verne's Robur le Conquérant (1866), which describes the rescue of shipwrecked sailors by an airship (balloon) named the Albatross. The first documented use of an air ambulance occurred during the Siege of Paris in 1870. when balloons were used to evacuate more than 160 soldiers from the besieged city.
 |
| MEDEVAC BLACK HAWK UH60 |
During the Great War, the first true Air Ambulance flight was made when a Serbian officer was flown from the battlefield to hospital by a plane of the French Air Service. Records kept by the French at the time indicated that, if casualties could be evacuated by air within six hours of injury, the mortality rate among the wounded would fall from 60 per cent to less than 10 per cent - a staggering reduction!
During the First World War air ambulances were tested by various military organizations. Aircraft were still primitive at the time, with limited capabilities, and the effort received mixed reviews. The exploration of the idea continued, however, and by 1936 an organized military air ambulance service was evacuating wounded from the Spanish Civil War for medical treatment in Nazi Germany.
The first recorded British ambulance flight took place in 1917 in Turkey when a soldier in the Camel Corps, who had been shot in the ankle, was flown to a hospital in a de Havilland DHH within 45 minutes. The same journey by land would have taken 3 days to complete. In Britain, sick passengers were ferried by air from the Western Isles of Scotland to the mainland in the early 1930s. The first such flight to be recorded was on May 14, 1933 when a fisherman suffering from a perforated stomach, with consequent risk of peritonitis, was flown from Islay to Glasgow's Western Infirmary in a DH Dragon owned by Midland and Scottish Air Ferries.
In Switzerland, with the increasing interest in winter sports during the early post World War 2 years, the use of air ambulances evolved from the increasing difficulties experienced in mountain rescue work. Initially fixed-wing aircraft were used, landing medical teams with equipment as close as possible to the injured parties so that rapid first aid treatment could be applied prior to evacuation.
To overcome a lack of suitable landing sites close to the incident in mountainous regions, it was even at one stage proposed to parachute medical personnel with equipment and sledges into the rescue area. Although training was undertaken, there is no documentary evidence to suggest that this technique was ever put into practice.
The first documented medevac by helicopter occurred during the second World War. In April 1944, a US Army Air Forces aircraft with three wounded British soldiers on board, was forced down in the jungle behind Japanese lines near Mawlu in Burma.A new US Army Sikorsky YR-4B helicopter, flown by Lt. Carter Harman, could carry only one passenger but, over 25-26 April 1944, four return trips were made.
Following the end of the Second World War, the first civilian air ambulance in North America was established by the Saskatchewan government in Regina, Saskatchewan, Canada. Back in the United States, 1947 saw the creation of the Schaefer Air Service, the country's first air ambulance service. Founded by J. Walter Schaefer, of Schaefer Ambulance Service in Los Angeles, Schaefer Air Service was also the first FAA-certified air ambulance service in the United States. Para-medicine was still decades away, and unless the patient was accompanied by a physician or nurse, they operated primarily as medical transportation services.
The first dedicated use of helicopters by U.S. forces occurred during the Korean War, during the period from 1950-1953. While popularly depicted as simply removing casualties from the battlefield (which they did), helicopters also expanded their services to moving critical patients to more advanced hospital ships once initial emergency treatment in field hospitals had occurred. On August 4, 1950, just one month after the start of the Korean War, the first rotorwing medical evacuation was performed with a bubble-fronted Bell 47 (as seen in the TV series M*A*S*H). The wounded were transported on basket stretchers attached to the top of the landing gear on the outside of the small helicopter (Figure 3-1). They were covered with blankets in a nearly futile effort to maintain body heat and prevent wound contamination. It is estimated that more than 20,000 injured soldiers were evacuated by helicopter. The World War II casualty/death rate of 4.5 deaths per 100 casualties dropped to 2.5 per 100 casualties during the Korean War. While there were some technological advances in medicine during that period, the improvement is largely attributed to use of the helicopter to evacuate patients to definitive care more quickly. The external litter, however, did not allow for medical care during transport.
The next major advance in AM transport occurred during the Vietnam War, where the Bell UH-1 helicopter was placed into operation. Affectionately known as the Huey, this aircraft was large enough to hold patients inside, where medical personnel could begin treatment during the flight to a field hospital. The mass deployment of these aircraft as medevac units reduced the average delay until treatment to one hour. The ability to carry patients inside the aircraft was a key element in the reduction of mortality and morbidity. Military medics performed procedures previously done only by physicians: they started central lines, inserted chest tubes, and sutured bleeding wounds. This care, coupled with the initiation of specialty hospitals for the treatment of different types of injuries, resulted in a reduction in the mortality rate to 1 death per 100 casualties.
The first known civilian application of a medical helicopter was in 1958 in Etna, California. Bill Mathews, a businessman, started a helicopter service to ferry patients for Dr. Granville Ashcraft, the town's only physician. The town druggist also used the helicopter to deliver drugs during emergencies.
By 1969, in Vietnam, the use of specially trained medical corpsmen and helicopters as ambulances led U.S. researchers to conclude that servicemen wounded in battle had better rates of survival than motorists injured on California freeways. This conclusion inspired the first experiments with the use of civilian paramedics in the world.
Two programs were implemented in the U.S. to assess the impact of medical helicopters on mortality and morbidity in the civilian arena. Project CARESOM was established in Mississippi in 1969. Three helicopters were purchased through a federal grant and located strategically in the north, central, and southern areas of the state. Upon termination of the grant, the program was considered a success and each of the three communities was given the opportunity to continue the helicopter operation. Only the one located in Hattiesburg did so, and it was therefore established as the first civilian air medical program in the United States. The second program, the Military Assistance to Safety and Traffic (MAST) system, was established in Fort Sam Houston in San Antonio in 1969. This was an experiment by the Department of Transportation to study the feasibility of using military helicopters to augment existing civilian emergency medical services. These programs were highly successful at establishing the need for such services.
Also, in 1969 the state of Maryland received a grant to purchase Bell Jet Ranger helicopters and started one of the nation's first medevac programs. The four helicopters, manned by paramedics, were strategically based throughout the state for quick response to emergency situations. When they were not carrying patients, the helicopters were used for law enforcement and traffic control.
On November 1, 1970, the first permanent civil air ambulance helicopter, Christoph 1, entered service at the Hospital of Harlaching, Munich, Germany. The first civilian, hospital-based medical helicopter program in the United States began operation in 1972. Flight For Life Colorado began with a single Alouette III helicopter, based at St. Anthony Central Hospital in Denver, Colorado. In Ontario, Canada, the air ambulance program began in 1977, and featured a paramedic-based system of care. The system, operated by the Ontario Ministry of Health, began with a single rotor-wing aircraft based in Toronto. An important difference in the Ontario program involved the emphasis of service. 'On scene' calls were taken, although less commonly, and a great deal of the initial emphasis of the program was on the interfacility transfer of critical care patients.
Mercy Flight WNY was established by Douglas H. Baker in 1981 as the first air-medical service in New York State and one of the first in the country. From day one, Mercy Flight WNY has maintained its independence of any hospital and is currently one of only a handful of remaining not-for-profit providers. The majority of other US programs are operated by either for-profit organizations or hospitals. (Right: Patient being loaded in the early 80's. Paramedic on left Margaret Ferrentino, was first female paramedic in NY State and is current Mercy Flight Vice-President/CFO.)
Helicopters continue to play a vital role in miltary medevacs. UH-60 Blackhawk helicopters have been used extensively in Iraq and Afganistan to medevac wounded soldiers from the battlefield. While both countries feature harsh desert environments that take their toll on helicopters, Afganistan's mountain peaks as high as 18,000 feet further complicate the mission. Because of the vast, mountainous terrain, evacuating casualties often extends beyond what doctors call the "golden hour": that crucial 60 minutes during which a traumatically-injured person has to reach a hospital before their survival chances plummet. So medics have begun doing emergency procedures inside helicopters that would normally wait for ER doctors.
The United States has some 200 operations whose services are paid for primarily by the patients and their insurance companies. As well as Switzerland, France, Austria, Italy Scandinavia and the former West Germany all have very successful versions of the helicopter-based EMS, the benefits of which have in some instances been particularly well-documented.
In Germany for example, there is now a network of helicopters which has evolved over the past twenty years to cover the entire country. Statistics which have been gathered over this period of time show:
- An average response time to the scene of the incident of just 10 minutes.
- Intensive care stays in hospital have been shorted by between five and seven days.
- There are 9% fewer wound infections.
- A significant reduction in the number of deaths during transport to hospital.
- Head injury mortality has been reduced by 15%.
Information from http://www.mercyflight.org/content/pages/medevac
Related

Related
Helicóptero BlackHawk como Ambulancia Aérea / BlackHawk Helicopter for Medical Evac / UH-60 A


Heli-operaciones
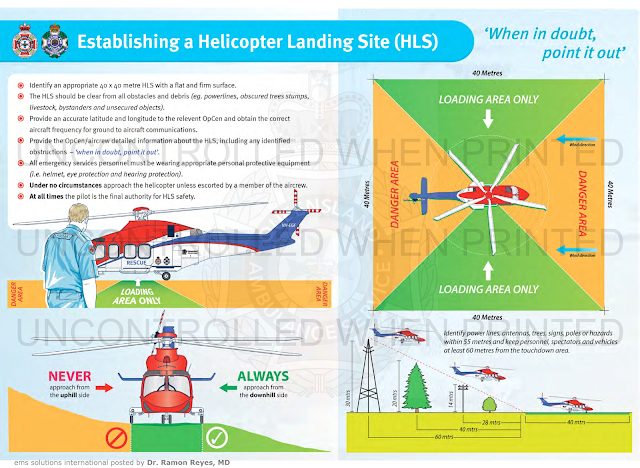
Estableciendo una Zona de Aterrizaje de Helicóptero
MEDEVAC / TACEVAC / CASEVAC / AROMEDICINA / TRANSPORTE AEROMEDICO https://emssolutionsint.blogspot.com/2019/08/medevac-tacevac-casevac-aromedicina.html #MEDEVAC #DrRamonReyesMD #AIR #AVION #HELICOPTERO #CASEVAC #TACEVAC #AEROMEDICAL
Estableciendo una Zona de Aterrizaje de Helicóptero
MEDEVAC / TACEVAC / CASEVAC / AROMEDICINA / TRANSPORTE AEROMEDICO https://emssolutionsint.blogspot.com/2019/08/medevac-tacevac-casevac-aromedicina.html #MEDEVAC #DrRamonReyesMD #AIR #AVION #HELICOPTERO #CASEVAC #TACEVAC #AEROMEDICAL
Fuente
Clinical Practice Manual (CPM)
EASA Welcomes New Rules On Mental Fitness Of Air Crews
EU Allows Two-Year Transition Period To Allow Airlines Time To Prepare For Implementation
The European Union has published new safety rules on air operations, including new provisions to better support the mental fitness of air crews.
The Regulation includes the following safety measures:
Support program: all pilots working for European airlines will have access to a support program that will assist and support pilots in recognising, coping with, and overcoming problems which might negatively affect their ability to safely exercise the privileges of their licence.
Alcohol testing: As an additional safety barrier, alcohol testing of pilots and cabin crew for all European and foreign airlines who fly into the territories of the European Union, has been added. Alcohol testing is already a well-established practice in some Member States and with this Regulation alcohol testing will now be extended to all EU Member States within the next two years.
Psychological assessment: European airlines will perform a psychological assessment of their pilots before the start of employment.
"These new European rules take up the proposals EASA made in its swift follow-up of the Germanwings Flight 9525 accident, in consultation with the wider aviation community," said EASA's Executive Director, Patrick Ky. "With these rules Europe introduces the right tools to safeguard the mental fitness of air crew. During the two year transition period, EASA will actively support European and international stakeholders in implementing this new Regulation’’.
As part of a total system approach, the new rules (so-called Air OPS Implementing Rules) complement the proposals EASA issued in August 2016, on the update of medical requirements for pilots (Part-MED).
The Regulation on mental fitness of air crew includes a two year transition period to allow airlines and Member States to prepare for the Regulation and to set up the necessary infrastructure to comply with the Regulation. EASA will issue Acceptable Means of Compliance and Guidance Material - AMC/GM in the form of a Decision- to support the implementation of the new rules and will work with Member States and industry to assist the implementation of the Regulation.
(Source: EASA news release)
http://www.aero-news.net/index.cfm?do=main.textpost&id=d9b49865-e80f-436a-ab58-adb32664306d

COMPARTIR: Mas 400 MANUALES Y LIBROS EN PDF GRATIS, sin trucos para descargar...
https://www.facebook.com/pg/DrRamonReyesMD/photos/?tab=album&album_id=620883388254594
Otra caída de helicóptero sanitario
Leer https://lnkd.in/eHghEBbb
Medical helicopter crashes while responding to scene of fatal crash

by STIER España
Recuerda que Stier Training Centre impartimos el curso BOSIET, tanto EBS como CA-EBS. Es un requisito indispensable para trabajar en plataformas offshore.
https://emssolutionsint.blogspot.com/2011/09/basic-offshore-safety-induction.html
¡También ofrecemos la teoría online!
En el BOSIET aprendemos de lucha contra incendios 🔥, supervivencia en mar 🌊, primeros auxilios🧑⚕️, emergencia en helicópteros 🚁e introducción a la seguridad en plataformas ⚓️.
GRUPO STIER
Teléfono +34 638 24 04 51
CONTACT
Las Palmas G.C. Head Office,
Juan Rejón 48 - 6º - 35008,
Las Palmas de Gran Canaria,
Spain
(+34) 928 97 10 43
Training Center,
Muelle de Taliarte s/n - 35214
Telde, Las Palmas de Gran Canaria,
Spain
(+34) 928 97 10 43
Por favor compartir nuestras REDES SOCIALES @DrRamonReyesMD, así podremos llegar a mas personas y estos se beneficiarán de la disponibilidad de estos documentos, pdf, e-book, gratuitos y legales..
Grupo Biblioteca/PDFs gratis en Facebookhttps://www.facebook.com/
Facebook
Pinterest
Twitter
Blog
Gracias a todos el Canal somos más de 1000 participantes en WhatsApp. Recordar este es un canal y sirve de enlace para entrar a los tres grupos; TACMED, TRAUMA y Científico. ahí es que se puede interactuar y publicar. Si le molestan las notificaciones, solo tiene que silenciarse y así se beneficia de la información y la puede revisar cuando usted así lo disponga sin el molesto sonido de dichas actualizaciones, Gracias a todos Dr. Ramon Reyes, MD Enlace al
Enlace a TACMED en WhatsApp https://chat.
Enlace a TRAUMA en WhasApp https://chat.whatsapp.
Enlace a Científico https://chat.
TELEGRAM Emergencias https://t.me/+sF_-
TELEGRAM TACMED https://t.me/CIAMTO
Grupo Biblioteca/PDFs gratis en Facebook
https://www.facebook.com/
Facebook
Pinterest
Twitter
Blog
Gracias a todos el Canal somos más de 1000 participantes en WhatsApp. Recordar este es un canal y sirve de enlace para entrar a los tres grupos; TACMED, TRAUMA y Científico. ahí es que se puede interactuar y publicar. Si le molestan las notificaciones, solo tiene que silenciarse y así se beneficia de la información y la puede revisar cuando usted así lo disponga sin el molesto sonido de dichas actualizaciones, Gracias a todos Dr. Ramon Reyes, MD Enlace al
Enlace a TACMED en WhatsApp https://chat.
Enlace a TRAUMA en WhasApp https://chat.whatsapp.
Enlace a Científico https://chat.
TELEGRAM Emergencias https://t.me/+sF_-
TELEGRAM TACMED https://t.me/CIAMTO
AVISO IMPORTANTE A NUESTROS USUARIOS
Este Blog va dirigido a profesionales de la salud y público en general EMS Solutions International garantiza, en la medida en que puede hacerlo, que los contenidos recomendados y comentados en el portal, lo son por profesionales de la salud. Del mismo modo, los comentarios y valoraciones que cada elemento de información recibe por el resto de usuarios registrados –profesionales y no profesionales-, garantiza la idoneidad y pertinencia de cada contenido.
Es pues, la propia comunidad de usuarios quien certifica la fiabilidad de cada uno de los elementos de información, a través de una tarea continua de refinamiento y valoración por parte de los usuarios.
Si usted encuentra información que considera errónea, le invitamos a hacer efectivo su registro para poder avisar al resto de usuarios y contribuir a la mejora de dicha información.
El objetivo del proyecto es proporcionar información sanitaria de calidad a los individuos, de forma que dicha educación repercuta positivamente en su estado de salud y el de su entorno. De ningún modo los contenidos recomendados en EMS Solutions International están destinados a reemplazar una consulta reglada con un profesional de la salud.mplazar una consulta reglada con un profesional de la salud.